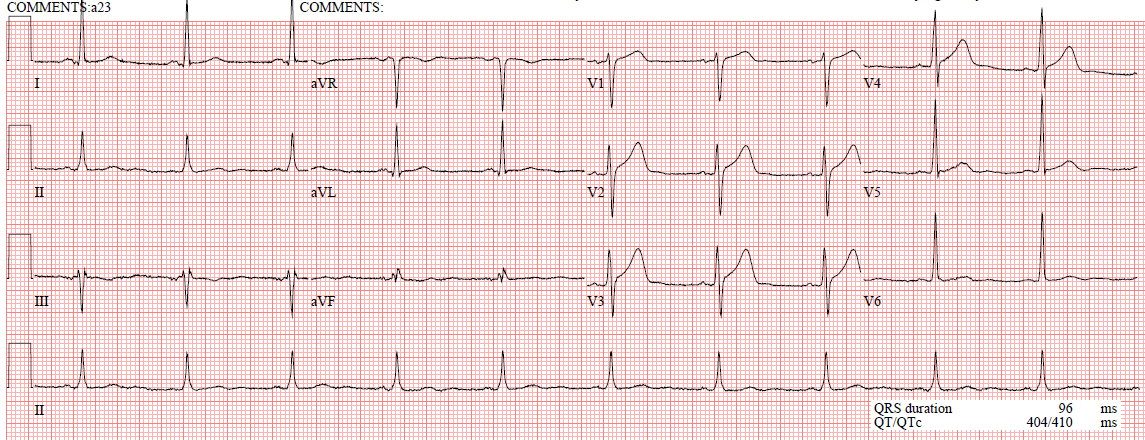
A male in late middle age with a history of RCA stent 8 years prior complained of chest pain. EMS recorded the following ECG:
 |
| What do you see? The computer read “Right Bundle Branch Block” |
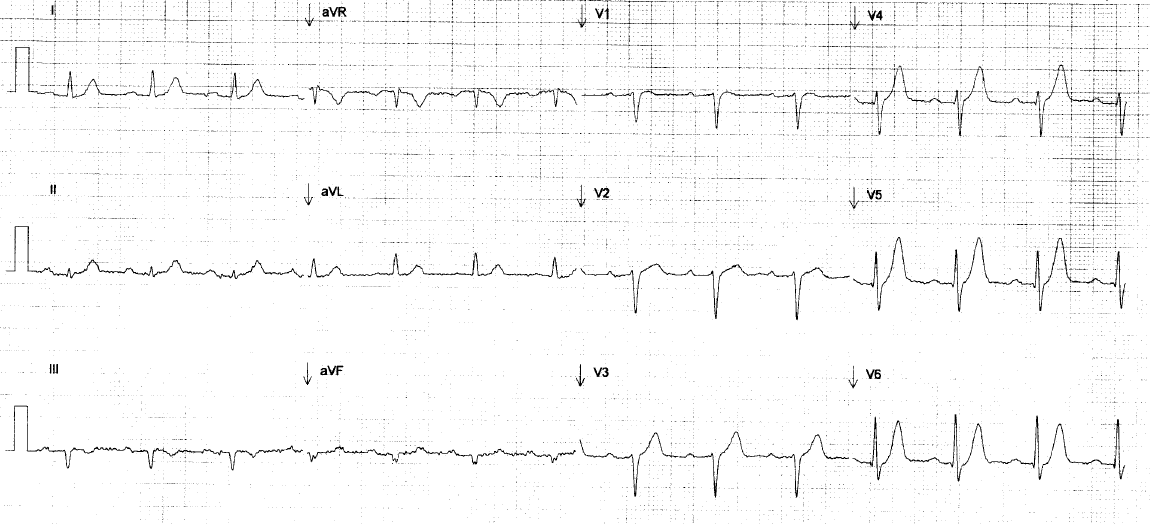
There is RBBB and LAFB, which can make it difficult to see the end of the QRS. I have annotated it here:
 |
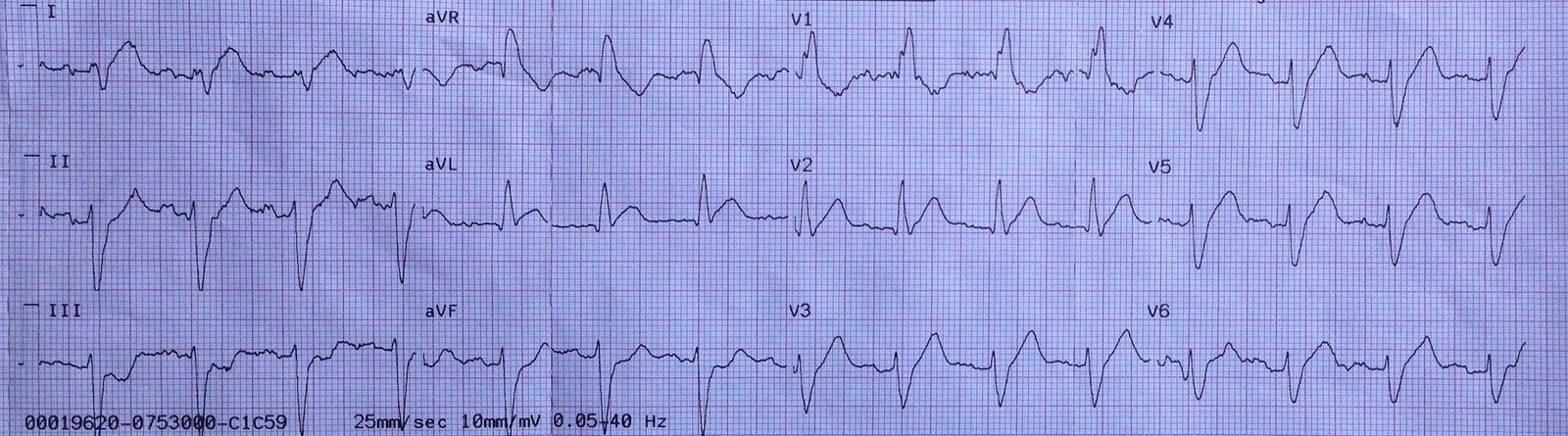
| The lines mark the end of the QRS and beginning of the ST segment. In RBBB, there should be no ST elevation, or minimal. In fact, V1-V3 should have some ST depression and T-wave inversion. In other words, the ST segment and T-wave should be discordant to (in the opposite direction of) the positive R’ wave [see the 2nd ECG of this post]. Here you can see abnormal (diagnostic) ST elevation and an upright T-wave in V2-V3, with diagnostic ST elevation in V4-V6 and in I and aVL, and with reciprocal ST depression in III and aVF. So this is diagnostic of proximal LAD occlusion. |
New RBBB + LAFB is a very bad sign. It is highly associated with proximal LAD occlusion and bad outcomes.
See this paper by Widimsky et al, which shows the high association of RBBB, especially with LAFB, with LAD occlusion. Furthermore, among 35 patients with acute left main coronary artery occlusion, 9 presented with RBBB (mostly with LAH) on the admission ECG.
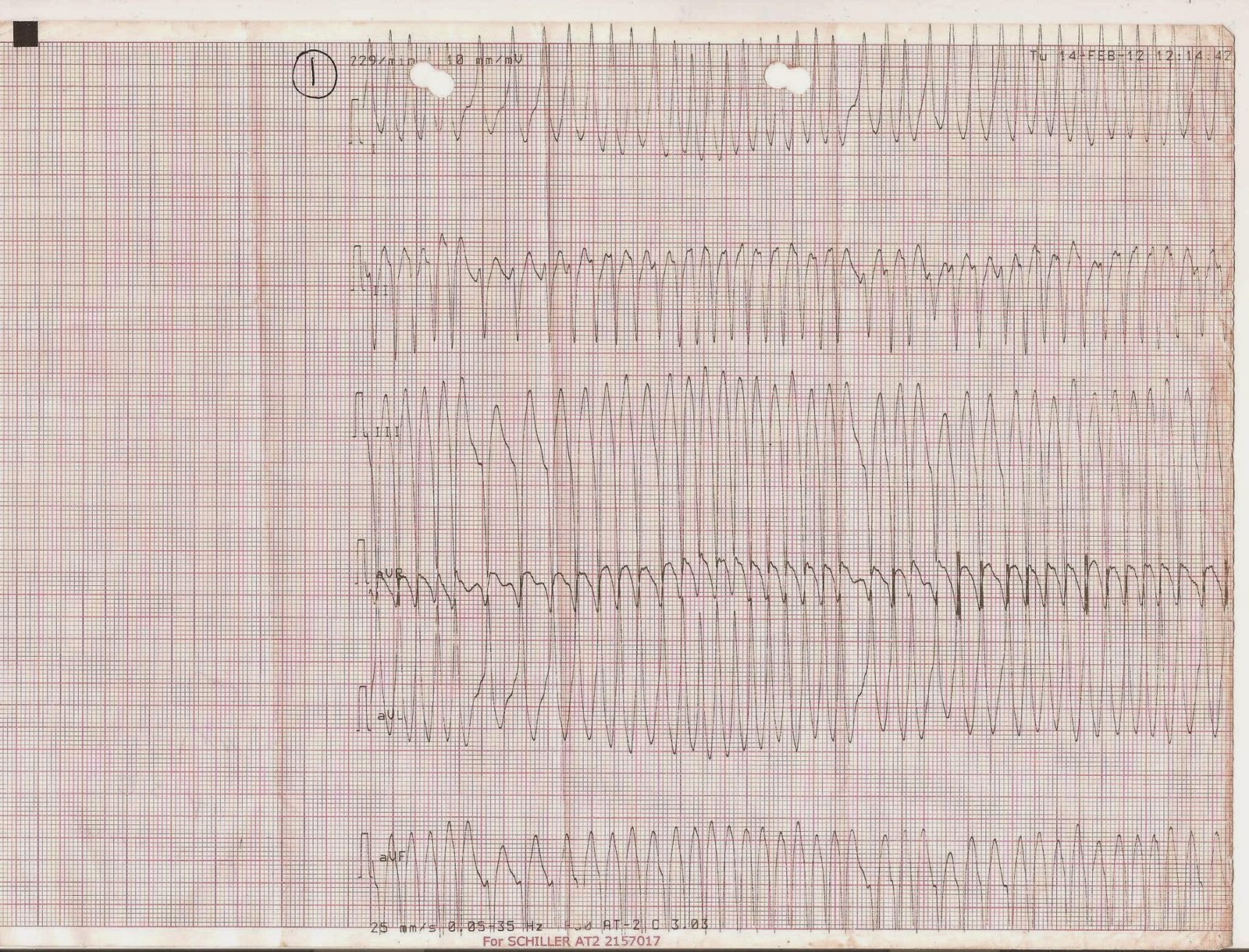
Here are three more dramatic cases that illustrate RBBB + LAFB
Case 1 of cardiac arrest with unrecognized STEMI, died.
Case 2 with 68 minutes of CPR and good outcome
Case 3 with LAD occlusion, cardiac arrest, could not be resuscitated
Case Progression
In order to keep patient confidentiality, I will only give the barest of follow up:
As the emergency physician was immediately assessing the patient, he had a v fib arrest. He could not be resuscitated in the ED but was taken to the cath lab while on LUCAS (mechanical) CPR, underwent successful PCI of a proximal LAD occlusion during chest compression, and after opening the artery, achieved ROSC (return of spontaneous circulation).
See this article by Widimsky: