We had a great pre-smaccGOLD EKG conference, with Louise Cullen moderating and featuring Ed Burns, Hussam Tayib, John Larkin, Roger Harris, Trevor Jackson.
The smaccGOLD conference was incredible and the conference will be in Chicago next year!! May 20-22, and I suspect there will be another EKG workshop the day before (May 19). I will be proposing an Emergency Cardiology workshop as well, so stay tuned for more.
Here is a great description of the conference: http://rebelem.com/social-media-critical-care-smacc/
Participants brought there own ECGs, and this was one:
An elderly woman smoker with a couple days of intermittent chest pain presented in shock. She had no past medical history and was on no medications. She was delirious and agitated and required ketamine for sedation.
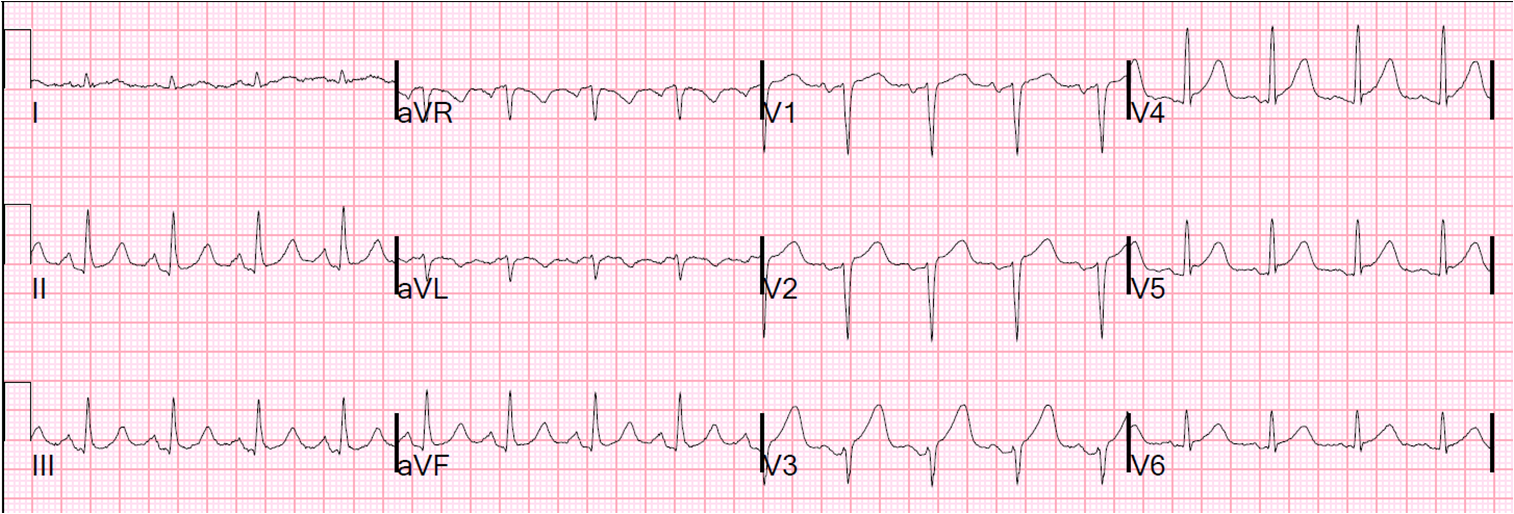
Here is her ECG:
 |
| Is this VT? Atrial Fib with RVR? Sinus? SVT? And what about the QRS? ST-T abnormalities? See below. |
Is this VT? Atrial Fib with RVR? Sinus? SVT? And what about the QRS? ST-T abnormalities?
Answer: Sinus Tach with junctional premature beats (thanks to Jason Roediger and K. Wang for pointing that out!–these are not PABs or PVCs), RBBB, LAFB. Subtle Antero-lateral ST elevation with inferior reciprocal ST depression. Q-wave in V1 (QR where there should be rSR’) suggests old or subacute MI. This is a very dangerous combination and is almost always due to LAD or left main occlusion.
Analysis
These very abnormal ECGs must be approached systematically unless you are very experienced and have instant morphology recognition. Even then you are best off verifying your recognition with a systematic approach:
1. rate
2. rhythm
2a. Fast?
i. P-waves?
ii. Regular or irregular?
iii. If irregular, regularly irregular or irregularly irregular?
iv. Wide or narrow?
v. Is it constantly fast? Sudden changes in rate? Gradual changes in rate?
vi. Are there premature beats?
2b. Slow?
i. Are there P-waves
ii. Do P-waves conduct?
iii. Are P-waves at regular intervals?
iv. Are QRS at regular intervals?
v. Are P’s and QRS associated? (no block)
vi. Are P’s and QRS dissociated? (block vs. dissociation only)
vii. Is QRS wide? (Escape or BBB)
3. QRS
3a. Axis
3b. Intervals (QRS, QT: look for LAFB, LPFB, RBBB, LBBB, IVCD)
3c. Voltage
3d. R-wave progression
3e. Q-waves
3f. S-waves
4.ST-T-U
4a. Voltage Proportional to QRS?
4b. Appropriate/Inappropriate discordance/concordance to QRS?
4c. T and QRS axis close to each other?
4d. ST axis?
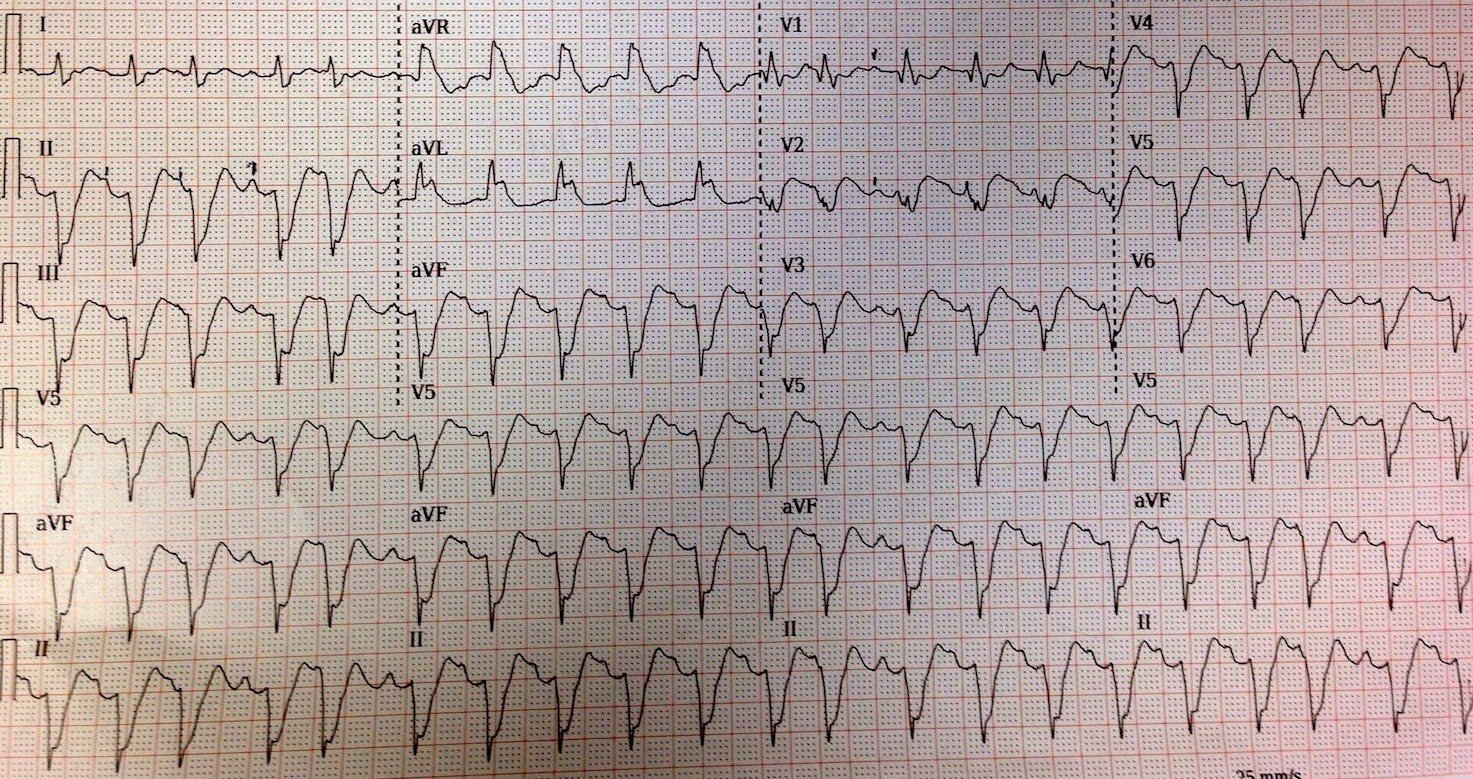
Here is an annotated ECG:
 |
| See full description below. Black arrows point to P-waves that are hidden in preceding QRS but do conduct. Red arrows point to easily seen P-waves. These are easily seen because they follow a premature beat which does NOT reset the sinus node. The blue arrow points to a P-wave that is hidden by BOTH the preceding T-wave and the onset of the following PVC. The green arrows point to premature beats. Are they PACs or PVCs? This is very difficult to ascertain: if PVCs, they have a remarkably similar morphology to the conducted (LAFB, RBBB) QRS; if PACs, where is the premature atrial activity and why does it not reset the sinus node? My conclusion is that they are PVCs that originate from near the posterior fascicle. |
Here is a more systematic analysis:
1. the rate is 120
2. one can see P-waves (black, red, and blue arrows)
3. P-waves are regular
4. QRS is irregular, but Regularly irregular, with beats 3, 5, 12, and 19 coming early (PAC vs. PVC vs. JPB. These are Junctional premature beats, as the QRS is identical to the normal QRSs and there is no visible atrial activity).
5. There is some P to QRS dissociation (also beats 3, 5, 12, and 19)
6. QRS is wide
QRS
Axis is left
End of QRS is where black lines are
QRS duration in about 160 ms
Q-wave in V1
There are Deep S-waves in II, III, aVF and V2-V6.
There is a large R-wave in aVL and V1
Thus, the QRS morphology is LAFB and RBBB
ST-T-U
The ST segment begins at the end of the QRS, at the black lines
There is ST elevation, see ST segment after black line in V2, V3, aVL
Outcome
Taken to cath lab and had a proximal LAD occlusion, arrested and was unable to be resuscitated.
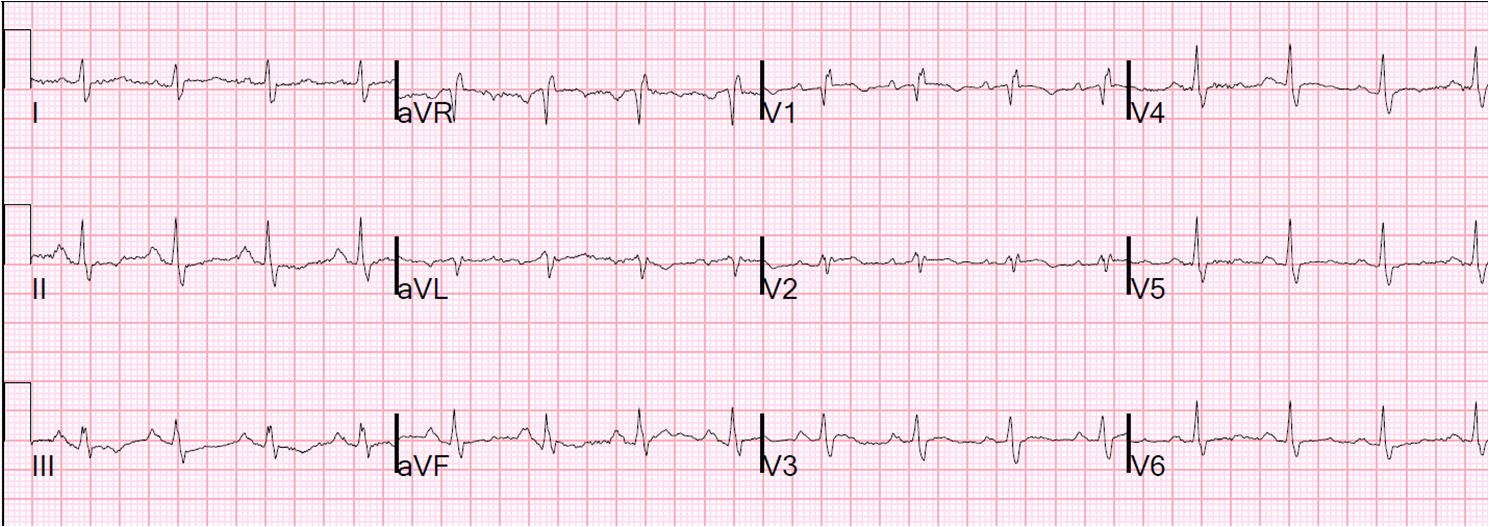
Here are two other similar ECGs:
First one (one of my most popular posts ever)
Second one (an incredible resuscitation with great outcome and also very frequently viewed)