A middle aged male had chest pain. There was suspicion of acute MI.
The initial ECG was texted to me:
 |
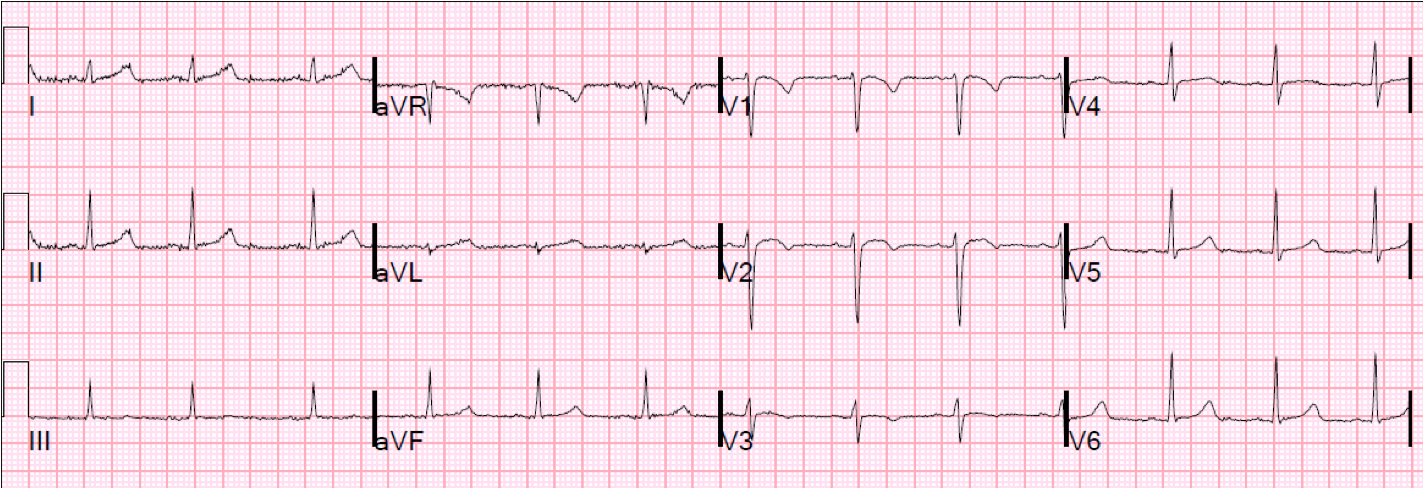
| The QTc is 423 ms. There is a large amount of ST elevation and Massive T-waves in V2 and V3, worrisome for LAD occlusion. However, there is also excellent R-wave progression. |
A repeat ECG was done a short time later:
 |
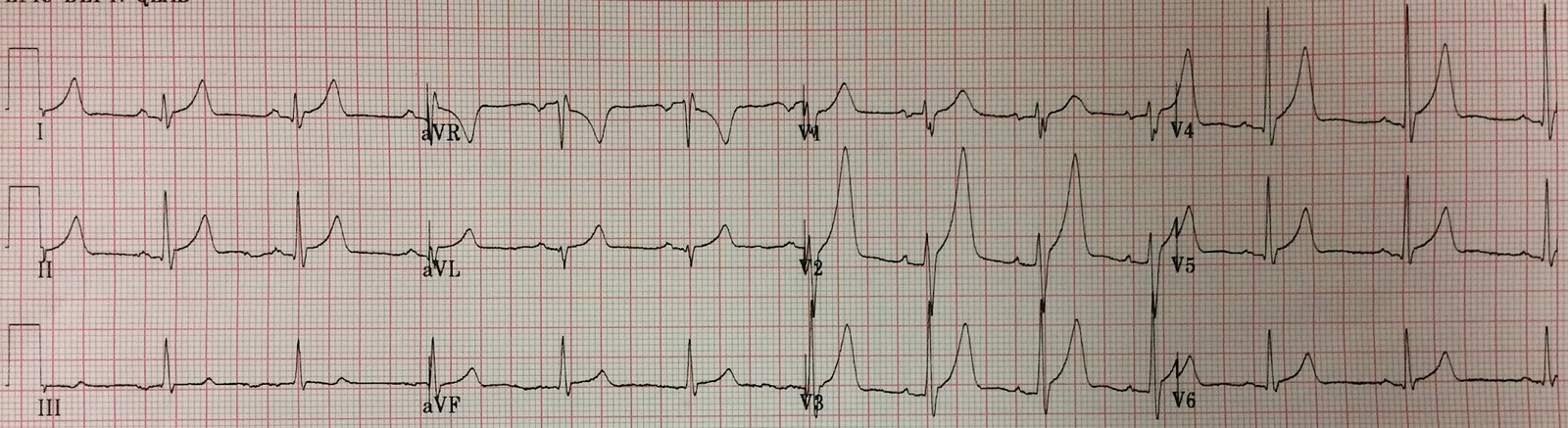
| No definite change. Computerized QTc is 399 ms. |
The potassium was 4.5 mEq/L.
Both of these ECGs are very worrisome for STEMI, but not diagnostic even though the second one meets criteria for STEMI (greater than 2 mm at the J-point in 2 consecutive leads). Early repolarization can look like this, however.
So the formula for differentiating acute LAD occlusion from Early repolarization was applied:
See sidebar for calculator:
 |
| The exclusions are CRITICAL (in red) |
Applying the formula to ECG 1, we get 22.025. This is about 97% sensitive for LAD occlusion at a cutoff of 22.0, and 92% sensitive at a cutoff of 23.4.
If we apply to ECG 2 (which has MORE ST elevation), we get 19.63 (very low).
This ECG is so worrisome that I would not be entirely convinced that this is not MI. But I would not activate the cath lab without more information if it is a strain on resources (nighttime, weekends, for instance).
A formal echocardiogram with contrast was done and showed no anterior or apical wall motion abnormality.
The patient ruled out for MI.
Learning Points:
1. When the differential is LAD occlusion vs. Benign Early Repol, the formula may help you to rule out STEMI
2. If it is STEMI, there will be a Regional Wall Motion abnormality. If the equation indicates Early repol and you don’t want to overuse scarce resources, then obtain an emergency high quality ultrasound to look for a wall motion abnormality.