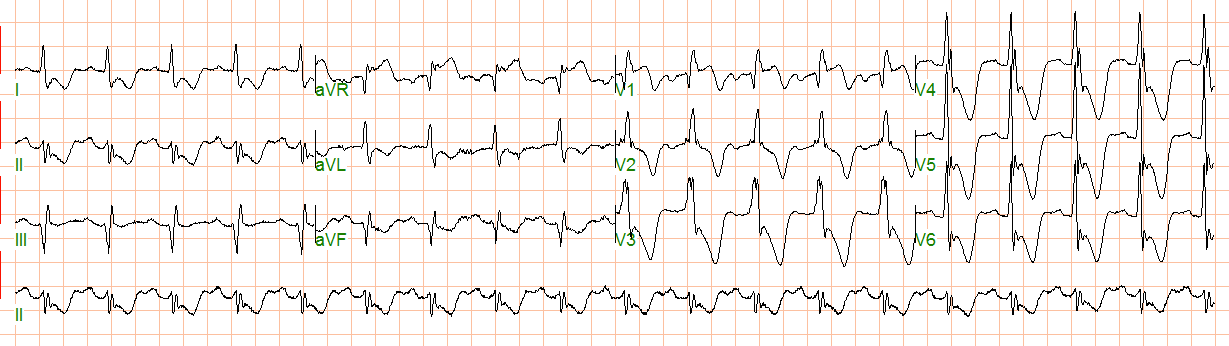
An elderly male complained of chest pain. Here is his ED ECG:
 |
| Inferiorly, there are Q-waves with minimal ST elevation and reciprocal ST depression in aVL. There is also subtle ST elevation in V3 and some ST depression in V5 and V6 Is this a subtle inferior MI? Subtle anterior MI? See below. |
Notice there is pre-excitation (WPW). The delta wave is negative in III and aVF (mimicking a Q-wave of MI). It is easiest to see in I and aVL, where the PR interval is also short. The PR interval is not short in every lead because the delta wave is not clearly visible in every lead. Look at lead II for instance.
Pre-excitation (an abnormality of depolarization) results in abnormal repolarization, often mimicking MI.
Whenever you see ST-T abnormalities (repolarization abnormalities), look to be certain that they are not simply a result of an abnormal QRS (depolarization abnormalities). Abnormal ST-T may be primary (due to a pathology such as ischemia) or secondary to an abnormal QRS.
Clinical course:
The WPW was recognized and serial ECGs remained the same. The patient ruled out for MI.
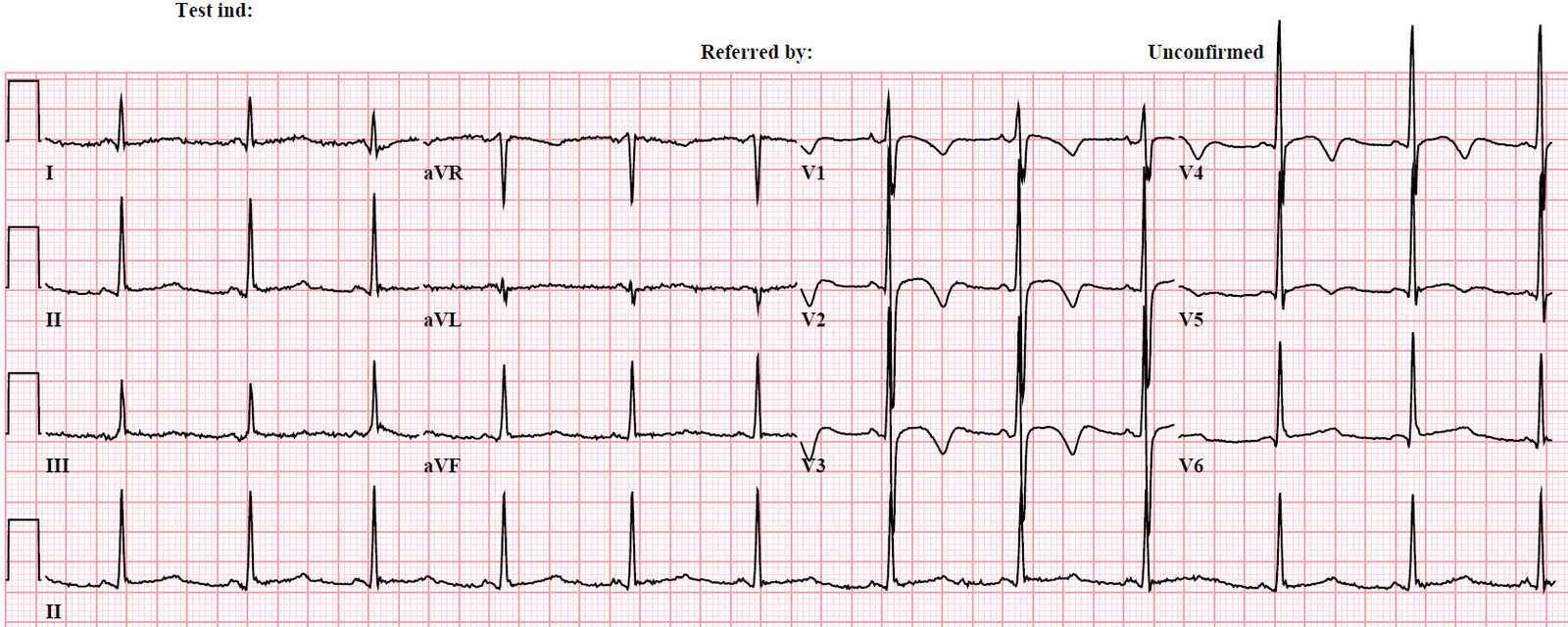
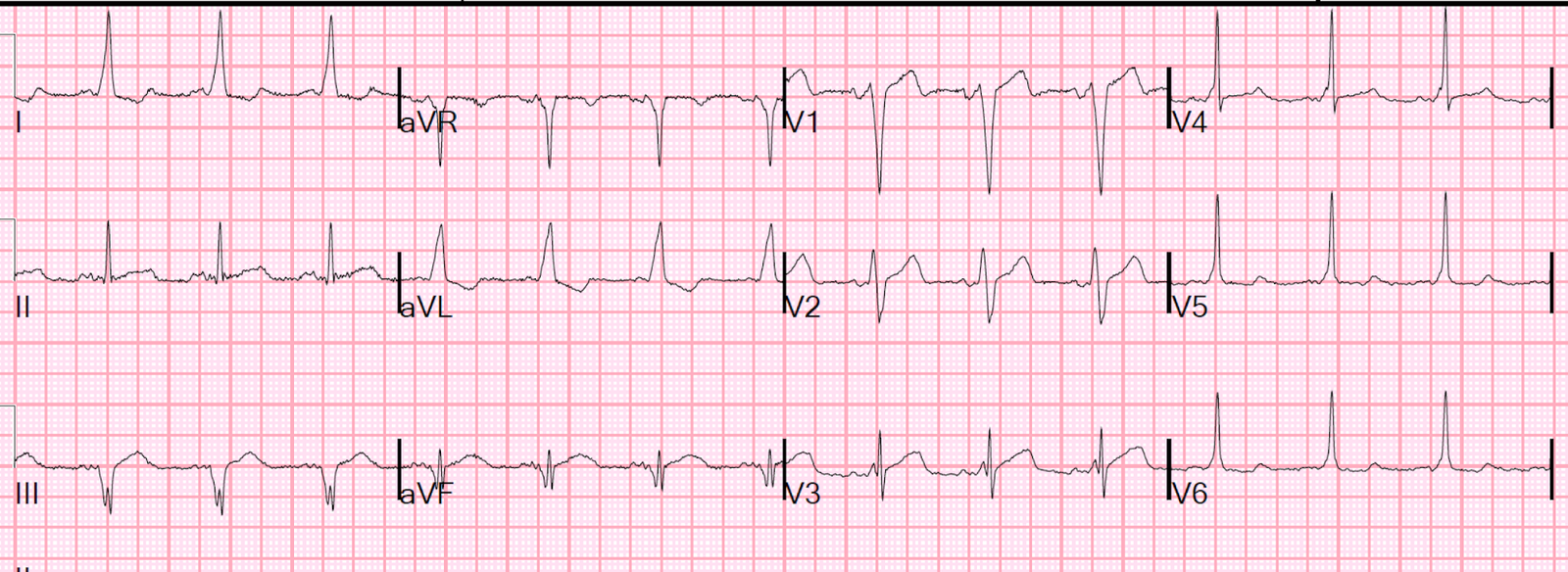
Here are several other examples of WPW mimicking MI: