This was inspired by an undergraduate named Harvey Pendell Meyers, who knows a heck of a lot about ECGs. How is that possible, as an undergraduate (like, not yet in med school)? You’ve got me on that one. But he sent case 5 which inspired this whole post.
WPW has abnormal depolarization through a bypass tract, manifesting as a delta wave. And like other ECG abnormalities that have abnormal depolarization (LVH, LBBB, RBBB, Brugada, hyperkalemia, and others), they also have abnormal repolarization. “Secondary repolarization abnormalities.” (Not primary, meaning the QRS is normal but repolarization is abnormal, as in ischemia).
Below are 5 cases:
Cases 1-3 are of WPW with secondary repolarization abnormalities that could mimic old or acute MI.
Case 4 shows a baseline WPW, then with MI superimposed on it.
Case 5 is a case in which WPW conceals acute MI.
Case 1.
 |
| WPW Mimics old inferior with acute posterior MI. Note that there are Q-waves in II, III, aVF and that the T-wave in these leads is upright. Note also that the WPW creates a wide QRS. A wide QRS results in repolarization (ST-T) that is discordant to the QRS, and proportionally so. (As in the Smith Modified Sgarbossa Criteria for LBBB and Paced Rhythm.) In this case, the ST depression is appropriately discordant in V1-V4 and not out of proportion. It was all due to WPW, not due to acute MI. |
In a study of 50 patients with inferior Q-waves due to WPW, 47 had an upright T-wave. The author, Ary Goldberger, suggests that in the presence of a delta wave and Q-wave, the T-wave should be discordant (opposite the Q-wave) as it is in this case, or at least isoelectric. He suggests that if it is concordant, then one should suspect inferior infarction. Accordingly, lateral QRS and T-wave should also be discordant.
Case 2.
 |
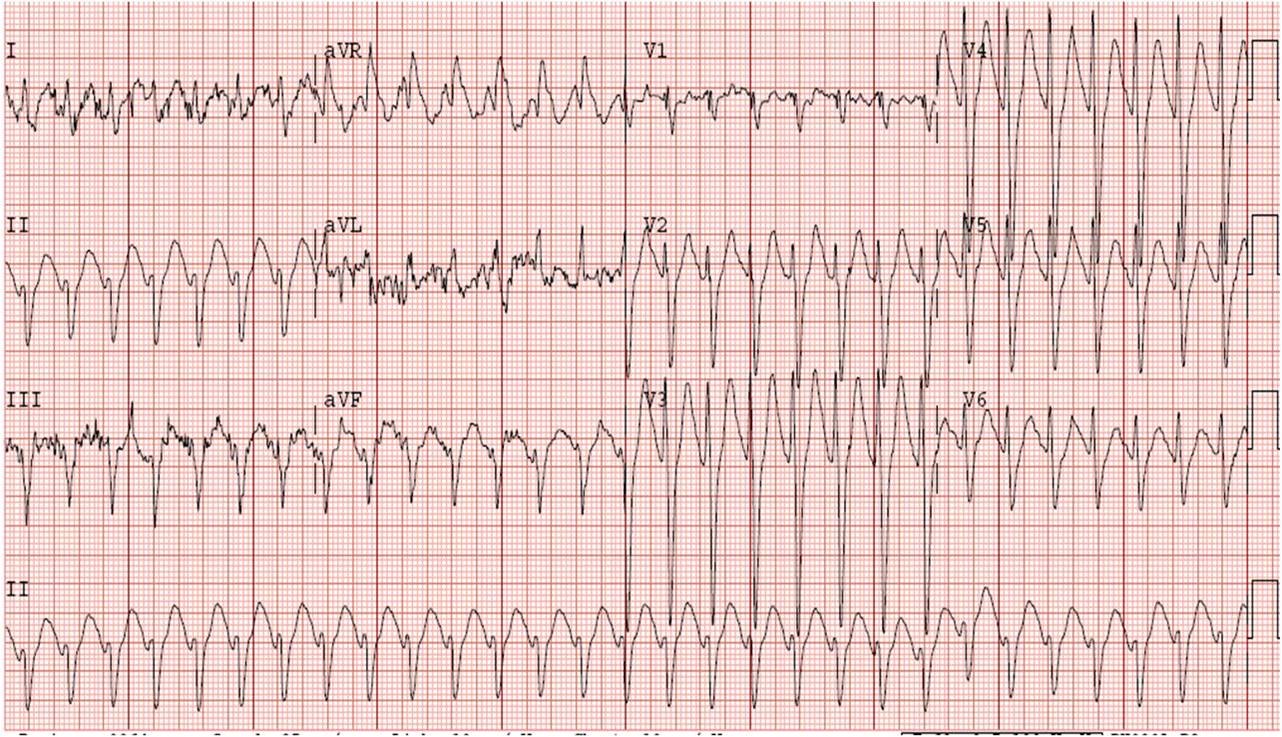
| WPW in this patient with Ebstein’s anomaly (post conversion for a fib with WPW) looks a lot like LBBB with anterior STEMI, but also with concordant T-waves in inferior and lateral leads. There is no definite Q-wave here, so one cannot apply Goldberger’s rule. Nevertheless, it is interesting to note that in limb leads, QRS and T-waves are concordant whereas in precordial leads they are discordant. These findings were all due to WPW. There was no myocardial infarction. |
Other
than the study on inferior Q-waves and its implications for diagnosis
of inferior MI, I know of no other studies assessing this phenomenon. I am not sure if, in WPW, there is a predictable pattern. Are the QRS and ST-T complex normally concordant or discordant? Not sure.
Case 3.
 |
|||||
| Anterior ST elevation is discordant to the S-wave and thus one can infer that it is due to WPW, not anterior STEMI. It does look somewhat like LBBB. Diffuse repolarization abnormalities are all due to WPW. ST segments are generally discordant here and T-waves are concordant. |
Case 4. ECG 1. Baseline ECG of a patient with WPW
 |
| This one has deep Q-waves in inferior leads with some minimal ST elevation and reciprocal depression in aVL. The T-waves are inverted, suggesting perhaps old MI? |
Case 4. ECG 2. The patient above presented with Chest pain and had this ECG recorded:
 |
| One might be tempted to attribute the ST elevation in II, III, aVF, and reciprocal ST depression in I and aVL, and ST depression in V2, as due to WPW. But this is excessive ST deviation for WPW. This is inferoposterior STEMI superimposed on the WPW. Having the old ECG (the one above) makes the diagnosis of acute inferoposterior STEMI easy. |
Now you’re ready for Case 5. A patient with onset of chest pain at 4AM presents to the ED at 0519.
ECG 1 (0519).
 |
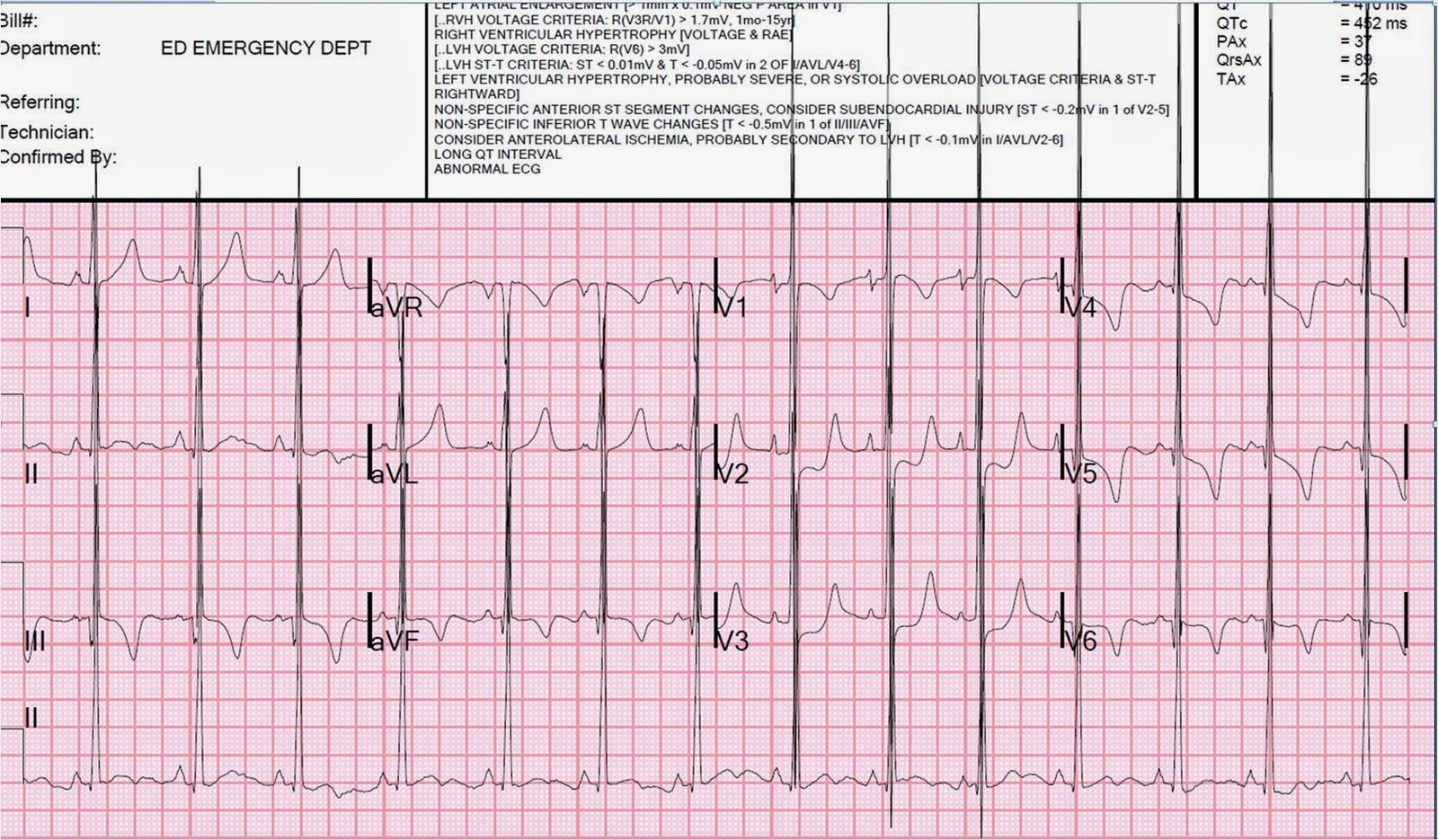
| Clearly there is WPW, with short PR interval and delta waves. There are deep QS-waves (negative delta waves) in III and aVF, with concordant T-waves and minimally concordant ST segment in V1 and V2. It is important to note that in a wide QRS, the ST-T should be discordant and the fact that it is not in V1 and V2 is worrisome for Occlusion MI in that territory. Similarly, T-waves are upright in I and aVL. Is there old or new inferior MI? There is ST depression in V3-V6. There are nonspecific ST and T-wave findings in V4-V6. Are these all due to WPW, or is there something hiding? |
ECG 2 (0543):
 |
| Minimal changes, but perhaps more concordant STE in V2 |
Neither of these ECGs, in my opinion, clearly show ischemia because WPW can so often mimic ischemia. However, the concordant ST-T is highly suspicious for Occlusion MI. The clinicians were worried and took the patient for an angiogram, which showed a 95% stenosis of the first diagonal with TIMI 2 flow. It was stented.
Post reperfusion ECG, 1330:
 |
| Many T-waves are now flattened or inverted since the last ECG. |
Day 2:
(Troponin I peaked at 31.38 ng/ml on Day 2)
 |
| Inferior T-waves are now clearly upright, lateral T-waves clearly inverted. So these discordant T-waves in III and aVF, and I and aVL appear to be the normal discordant T-waves that one finds when there are inferior Q-waves due to WPW. This appears to be a case of pseudonormalization of T-waves, but it is not true pseudonormalization because it is not from re-occlusion, but rather from reperfusion. In other words, after reperfusion, the T-wave vectors are in the expected direction for WPW, not inverted from normal as is common in reperfusion. |
Day 3, after ablation of accessory pathway:
 |
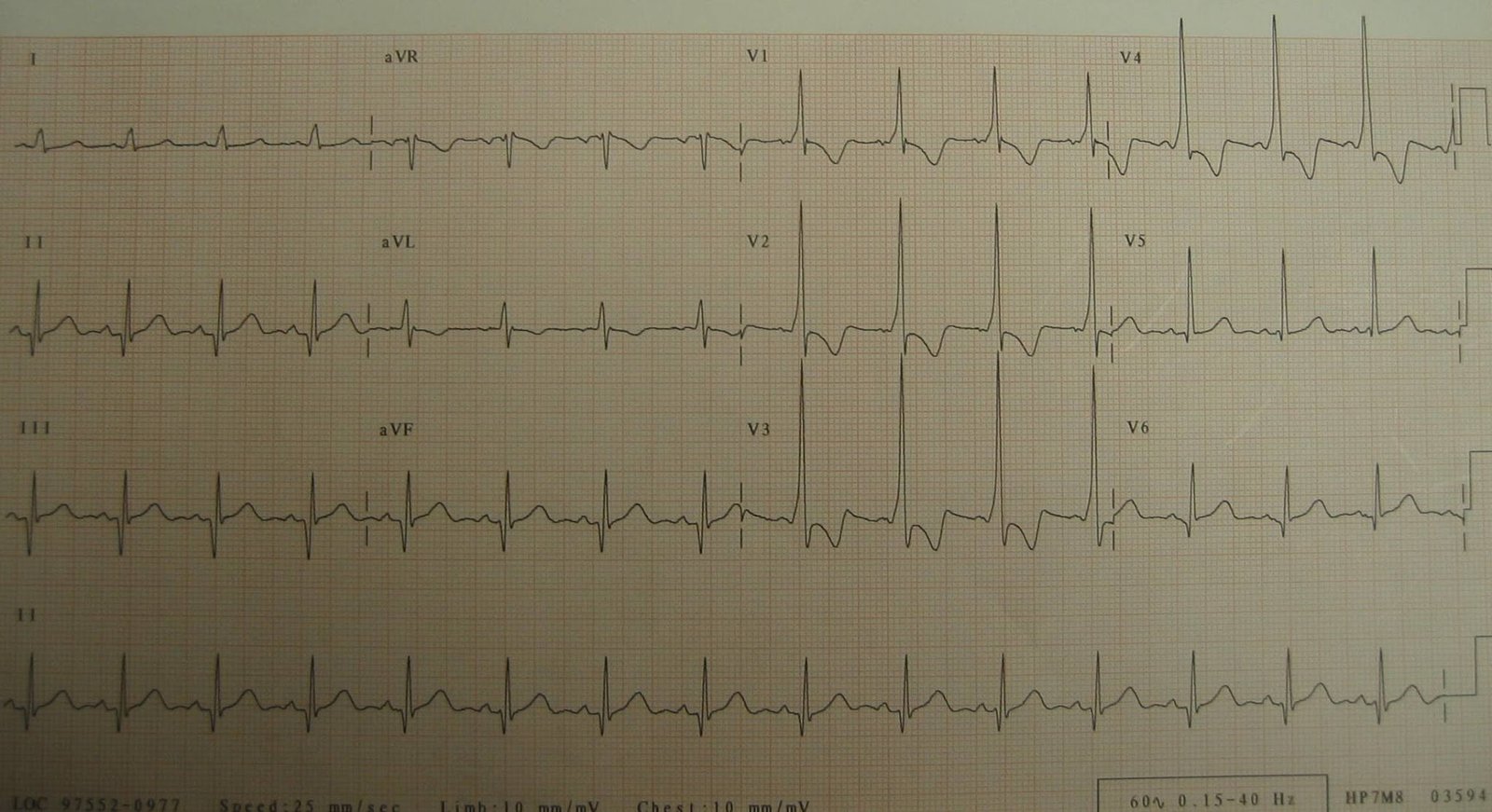
| QRS is normalized except for Q-waves in I and aVL (due to the lateral AMI suffered on this occasion). Interestingly, the T-waves are inverted in III and aVF, but not in I and aVL; that is to say that there are apparently no lateral reperfusion T-waves. There are large T-waves in V2 and V3 which may represent posterior reperfusion T-waves (or early repol, but without a comparison from prior non-WPW ECG, this is uncertain). |
Learning points:
1. WPW alters both depolarization and repolarization and can both mimic and obscure acute MI.
2. In WPW with inferior Q-waves, the T-wave is usually upright (discordant).
3. In WPW with inferior Q-waves, a concordant T-wave should raise suspicion for MI, either old or new.
4. I am uncertain as to whether there are other concordance and discordance rules that may help decipher ischemia in the presence of WPW.