Case
A 55 year old male heavy smoker presented with agonising chest pain and this ECG:
 |
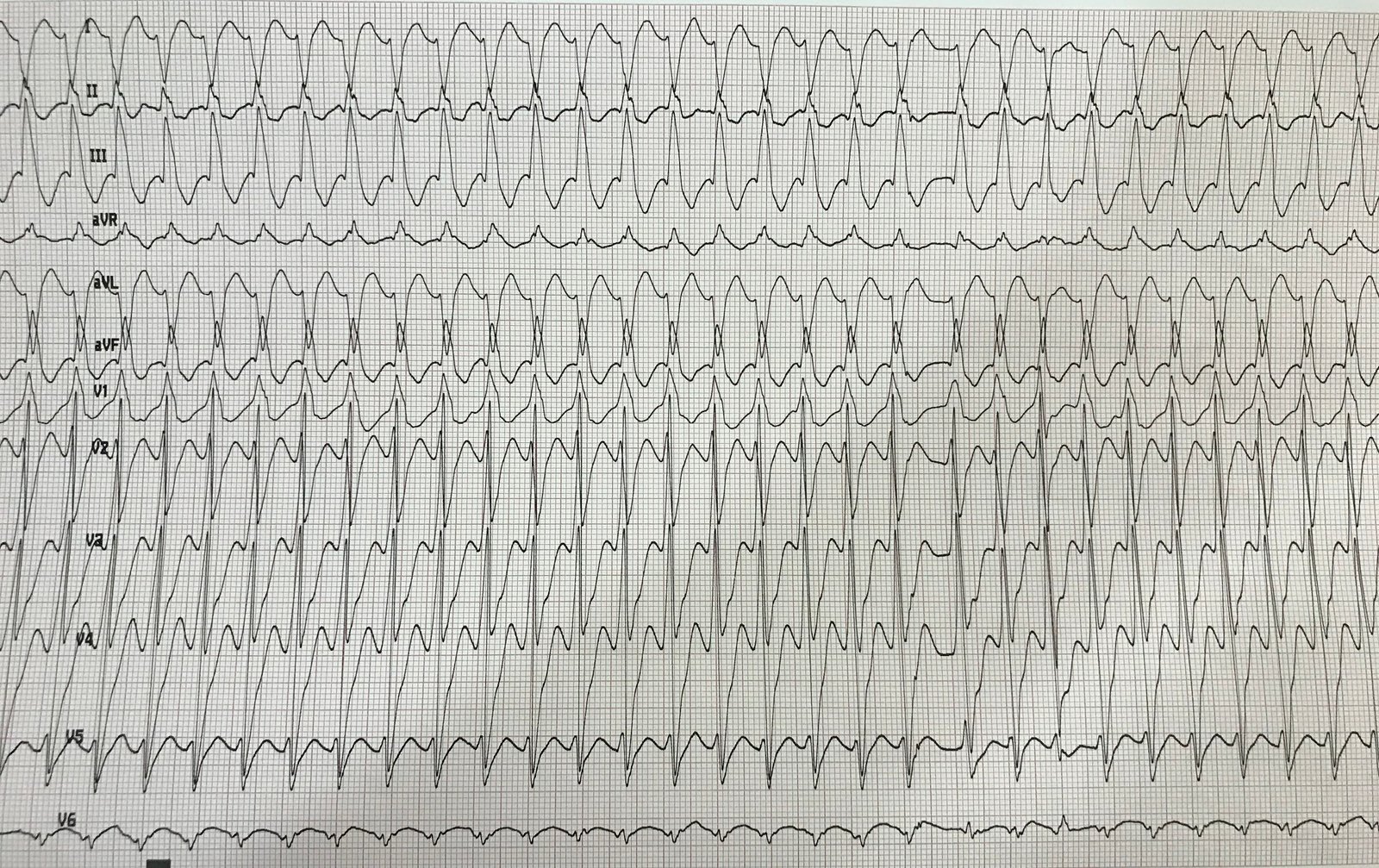
| There is sinus rhythm.
There is left bundle branch block (LBBB) There is no concordant ST elevation. The highest ST/S ratio is in V3, at approximately 4.5/24 = 0.19 See this post: A Fascinating Demonstration of ST/S Ratio in LBBB and Resolving LAD Ischemia |
The mean maximal ST/S ratio in non-ischemic LBBB is about 0.11. So 0.19 (19%) is abnormal.
In our validation study of the Modified Sgarbossa Criteria for diagnosis of acute coronary occlusion, we found that it performed similarly well using a cutoff of 20% or 25%:
Sensitivity and Spec at 20%: 84% and 94%
Sensitivity and Spec at 25%L 80% and 99%
So at a ratio of 0.19, there is still a high probability of occlusion.
I was sent this ECG by Facebook messenger, and asked my interpretation. Here is my response:
“V3 is suspicious for excessive discordance. I would say it does not look like an acute STEMI, but I could be wrong.”
The patient received thrombolytic therapy.
An angiogram was done after thrombolysis:
It showed moderate diffuse coronary disease and no thrombus.
LAD: mid segment moderate disease
OM: mid segment moderate lesion.
OM2: ostial moderate lesion
Ramus: moderate mid segment lesion
RCA: diffuse disease mid to distal, moderate lesion
The angiogram was considered to be “negative” for a culprit.
An ECG was repeated:
 |
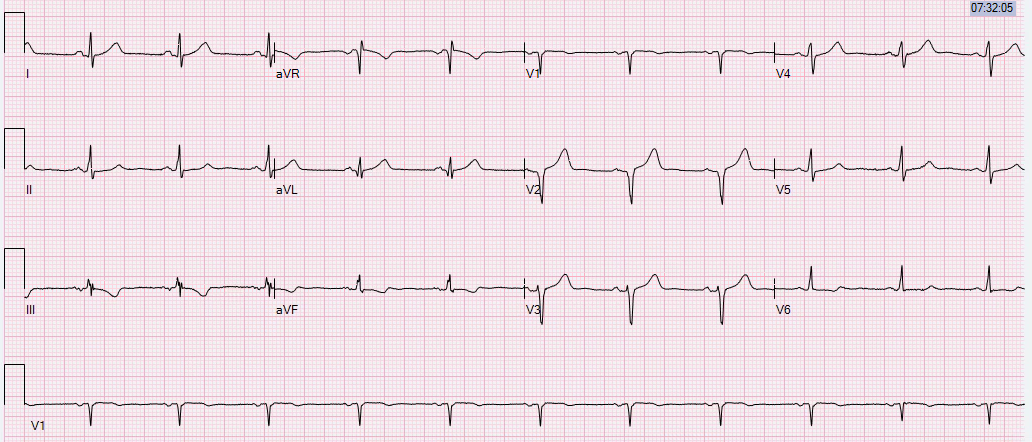
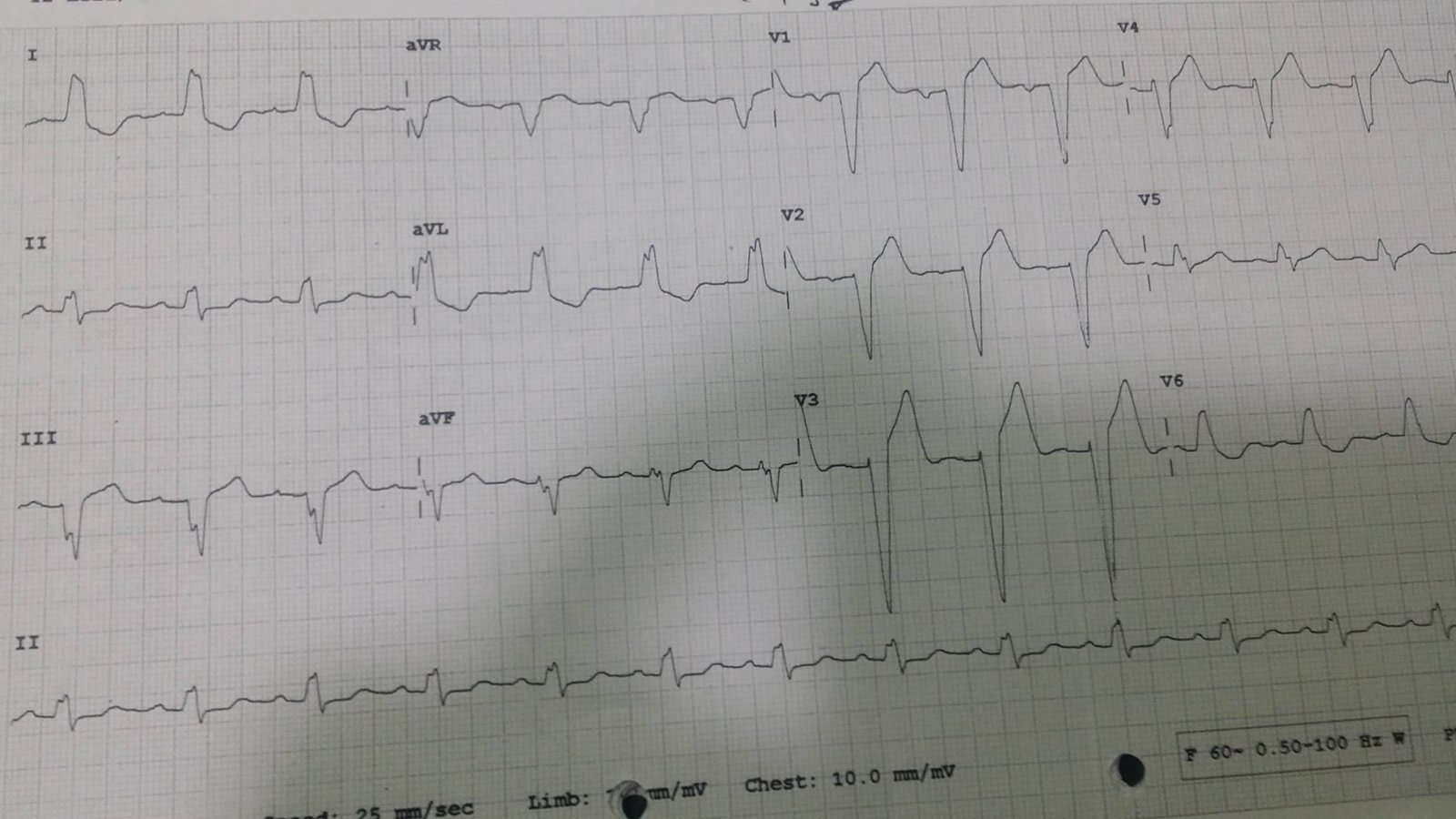
| LBBB is resolved. There is T-wave inversion in V2 and V3 highly suggestive of Wellens’ waves This represents LAD reperfusion |
An echo was done:
There were septal, apical, and anterior wall motion abnormalities.
Troponins
–(high sensitivity troponin I BiomerieuxVIDAS TNHS):
99% reference = 19 ng/L (%CV = 7% at this level)
LoD = 2 ng/L
Initial: 13 ng/L (detectable, but still below the 99%)
Followup: 38 ng/L (above the 99% and with a significant rise)
Here is the manufacturer’s chart for interpretation:
 |
| You can see that a rise in high sensitivity troponin of greater than 10 ng/L is a “rule in.” |
Even with a “negative” angiogram, the weight of evidence heavily favors LAD occlusion at the time of the ECG:
1. There was excessive discordance, even if it did not meet the 20% or 25% cutoff
2. There was coronary disease, even if no thrombus; thrombus would likely be lysed by tPA
3. The followup ECG (most important) was consistent with reperfusion of the LAD
4. There were corresponding wall motion abnormalities.
5. The high sensitivity troponin had a diagnostic delta, even though the absolute level was minimally elevated
Learning points
1. The cutpoints of 20% and 25% for the Modified Sgarbossa criteria maximize specificity, but are not fully sensitive for acute coronary occlusion. Every case must be evaluated carefully.
2. Not all ACS has a clearly visible culprit.
3. The best way to assess whether ST elevation represents ischemia is to look at followup ECGs. If the ST elevation resolves or evolves, then it is ischemic, even with all negative troponins!
See my last case: