
This 38 yo male presented with chest pain with activity for 4 days, worse on the day of presentation, and associated with SOB. He has a h/o Renal failure and has a transplant, lately struggling with CMV infection. His exam was negative. Here is the ECG:
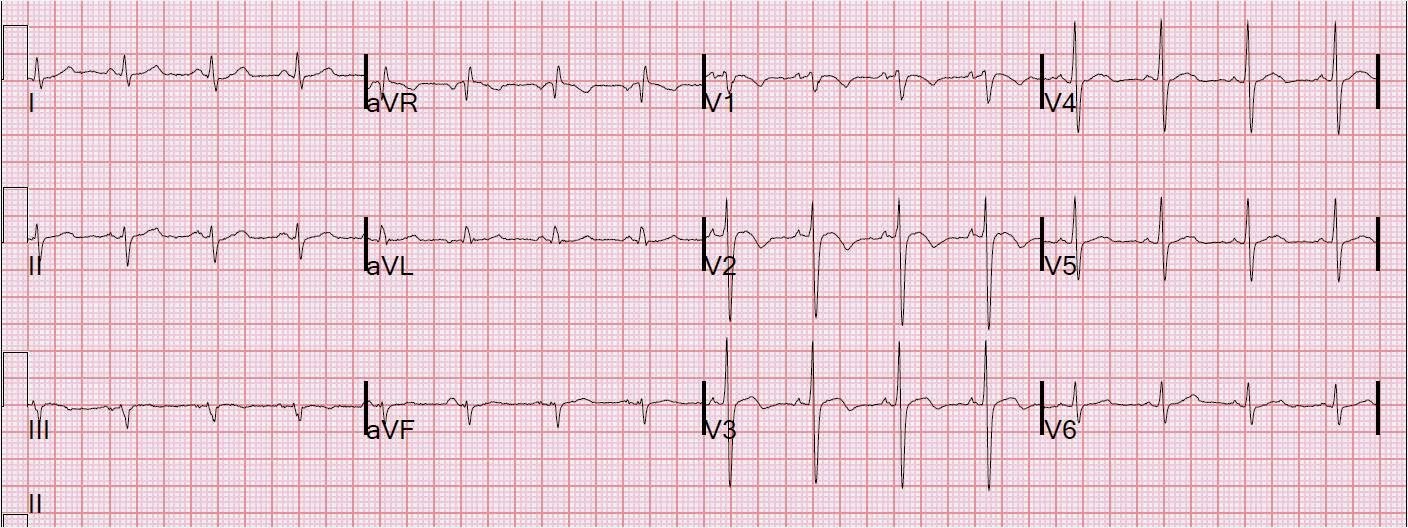 |
| There is sinus rhythm at a rate of about 100 (faster than normal for ACS). There is T-wave inversion in V1-V3, with some inversion also in lead III. |
The patient had an initial troponin I of 0.22 ng/ml (+) and an NT-proBNP of 3200 ng/ml (elevated). He was diagnosed with NSTEMI and admitted to the hospital on heparin.
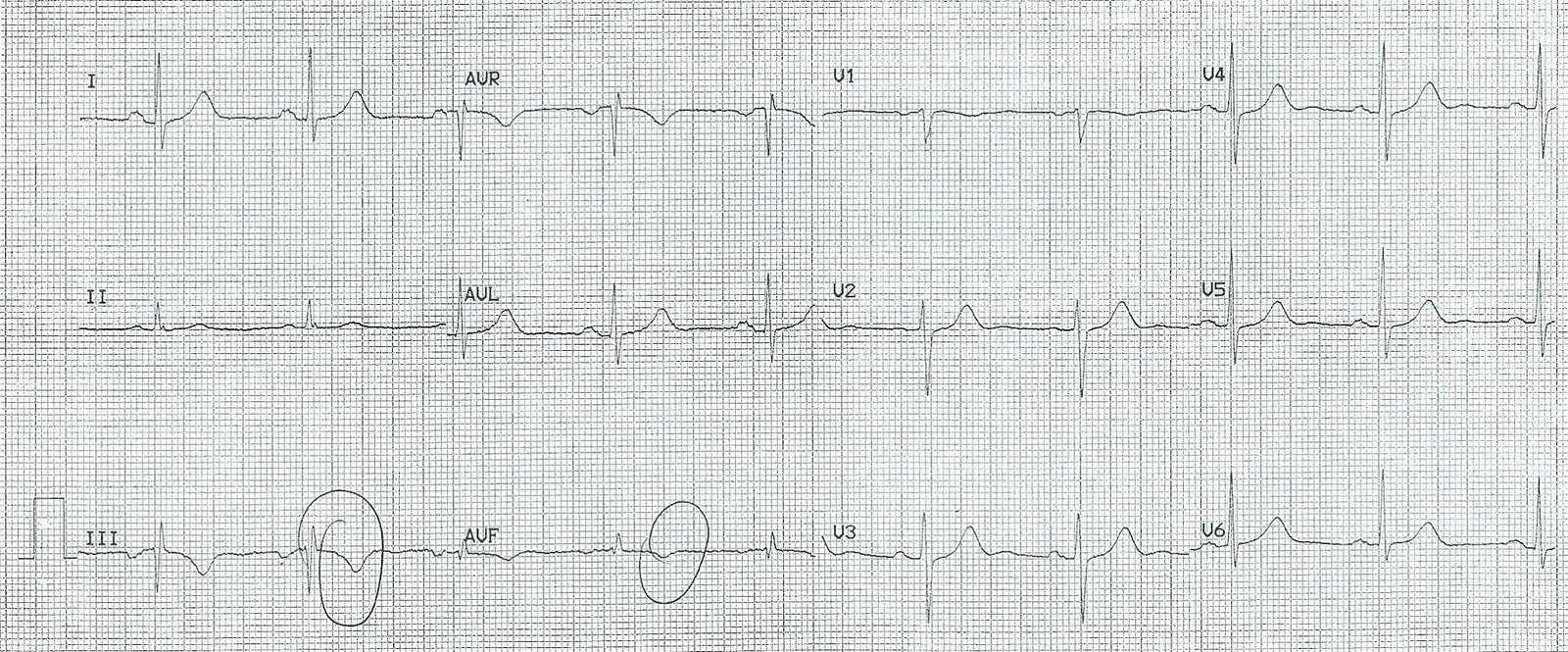
Here is a quote from this study, “negative T waves in leads III and V1 were observed in only 1% of patients with ACS compared with 88% of patients with Acute PE (p less than 0.001). The sensitivity, specificity, positive predictive value, and negative predictive value of this finding for the diagnosis of PE were 88%, 99%, 97%, and 95%, respectively. In conclusion, the presence of negative T waves in both leads III and V1 allows APE to be differentiated simply but accurately from ACS in patients with negative T waves in the precordial leads.”
Later, the patient had an echocardiogram which showed hyperdynamic LV fct (EF = 80%) and a dilated RV. PE was diagnosed by CT, with bilateral pulmonary emboli.
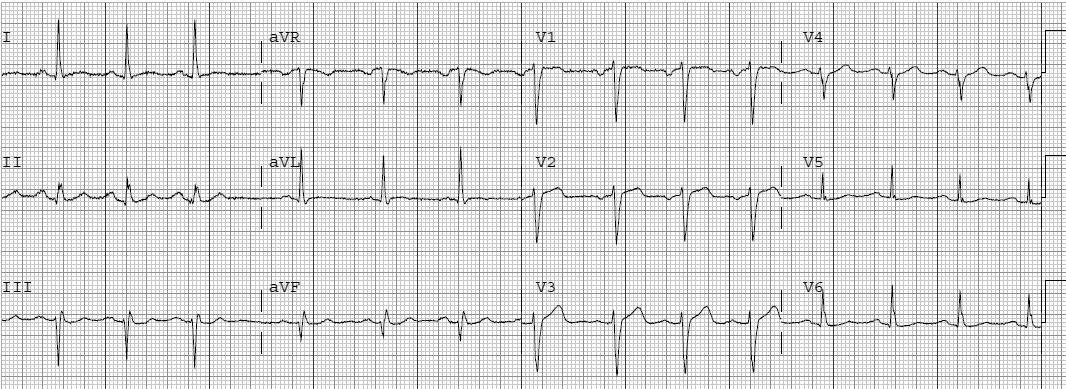
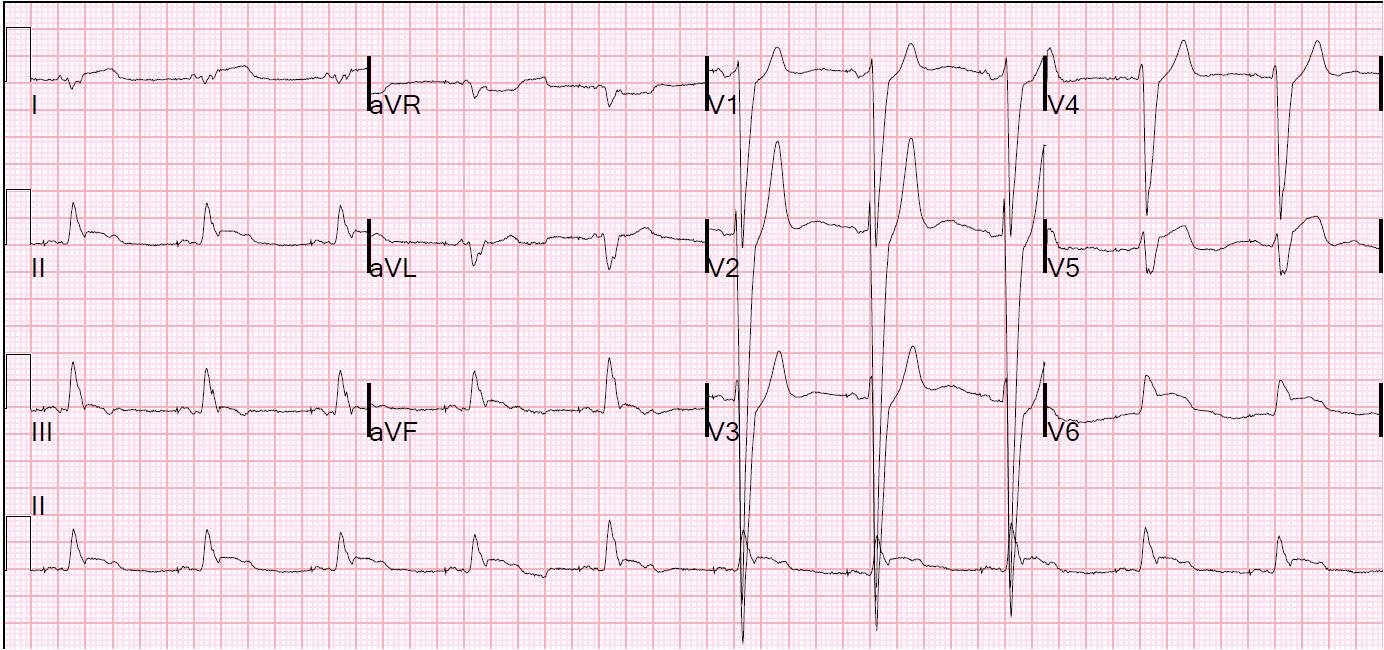
If this were ACS, it would be Wellens’ syndrome, and this just does not look like Wellens’ (difficult for me to explain why, but compare with other Wellens’ cases on this blog).
Compare with a classic Wellens’ with biphasic T’s:
Anterior T-wave inversion, when accompanied by T-wave inversion in lead III, especially if tachycardic, should make you think of PE. A simple emergency physician performed bedside ultrasound would have confirmed this. Troponin will not help you in this diagnosis because, when there are T-wave inversions in either situation, the troponin is positive.

{kind=link}