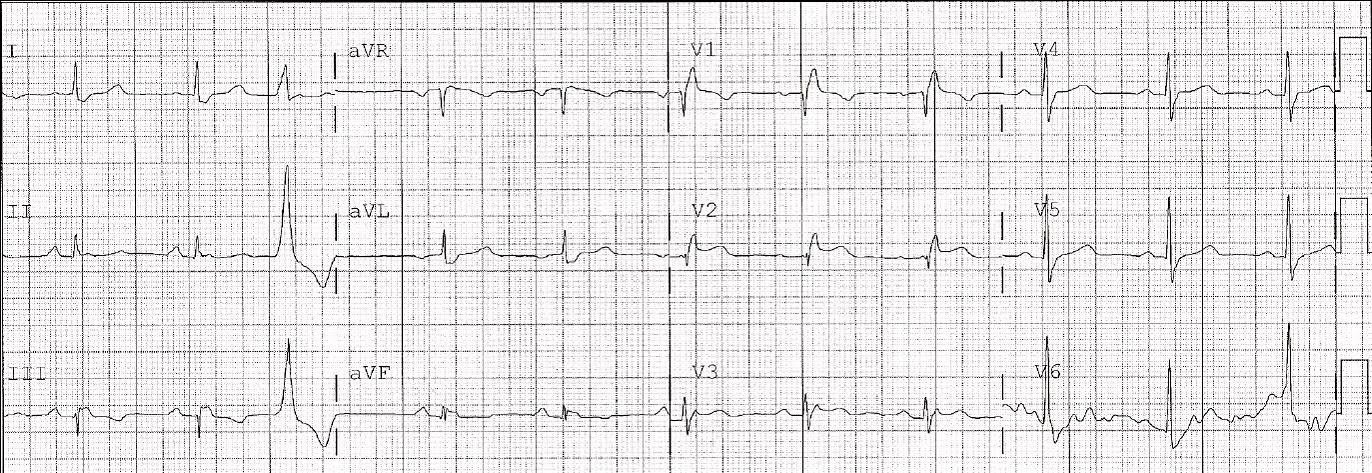
This patient presented with diabetic ketoacidosis. The physicians were reluctant to start insulin until they knew that the potassium was not too low. They had difficult IV access. This EKG was recorded:
There is sinus rhythm and a normal QRS. But repolarization is abnormal: there is scooped ST depression in I and aVL; there is a very prolonged QT interval (I measure a QT of 440 ms and QTc of 580 ms, though the computer got it very wrong at 440 ms); there are prominent U-waves (the bump between the T-wave and p-wave) in V2-V5.
The ECG is pathognomonic of hypokalemia. When the level returned, it was 2.3 mEq/L.
In a derivation study (which we have submitted only as an abstract so far) of ECGs of patients with hypokalemia vs. controls, in which interpreters were blinded to the K, we found very high sensitivity and specificity for a K less than vs. greater than 3.0 with any one of QTc of 450 ms or prominent U-waves or a subjective reading of hypokalemia.