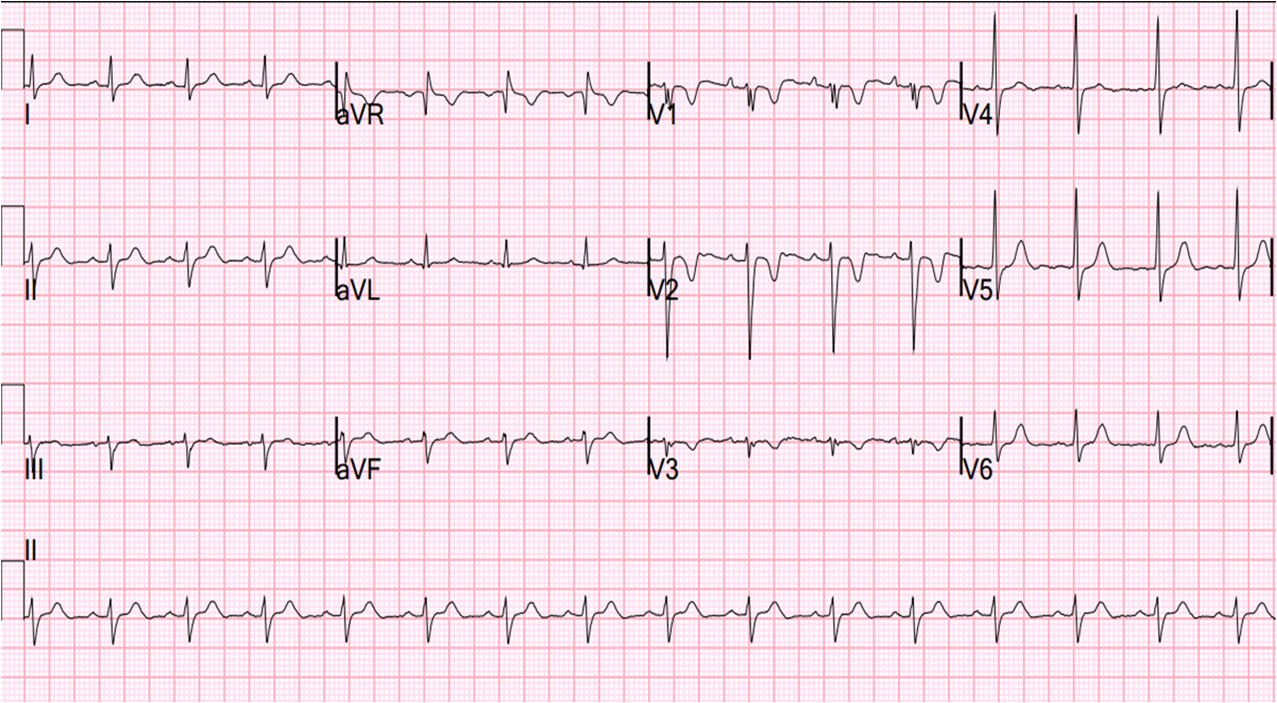
A male in his 40’s with no previous cardiac history had presented to a clinic recently with chest burning, had a nondiagnostic ECG, and was diagnosed with reflux. He presented to an ED with 2.5 hours of chest burning a few days later. His BP was 152/84. Here is the initial ECG:
 |
| Sinus rhythm, Q-wave in III with minimal ST elevation and minimal ST depression in I and aVL. There is a suspiciously minimally biphasic T-wave in V6. This is a nonspecific ECG. |
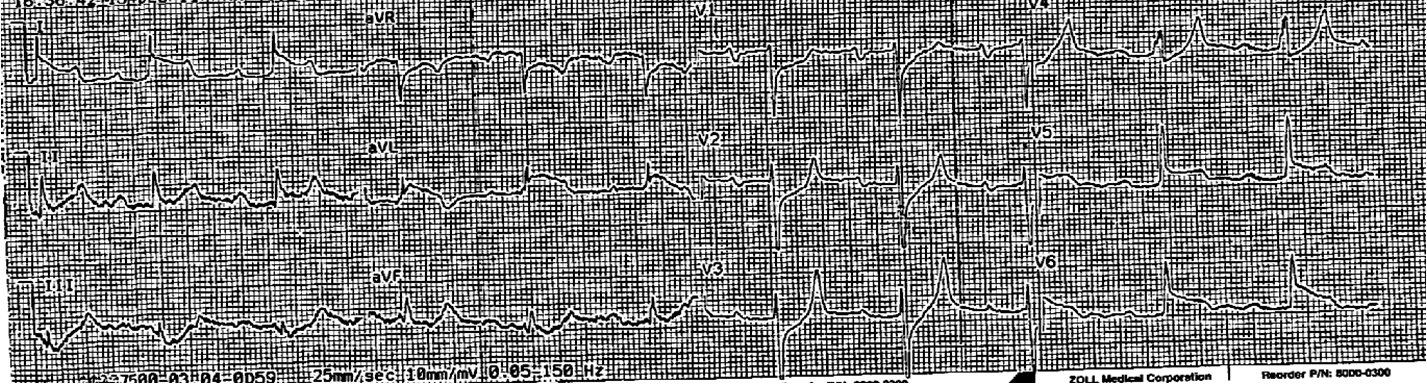
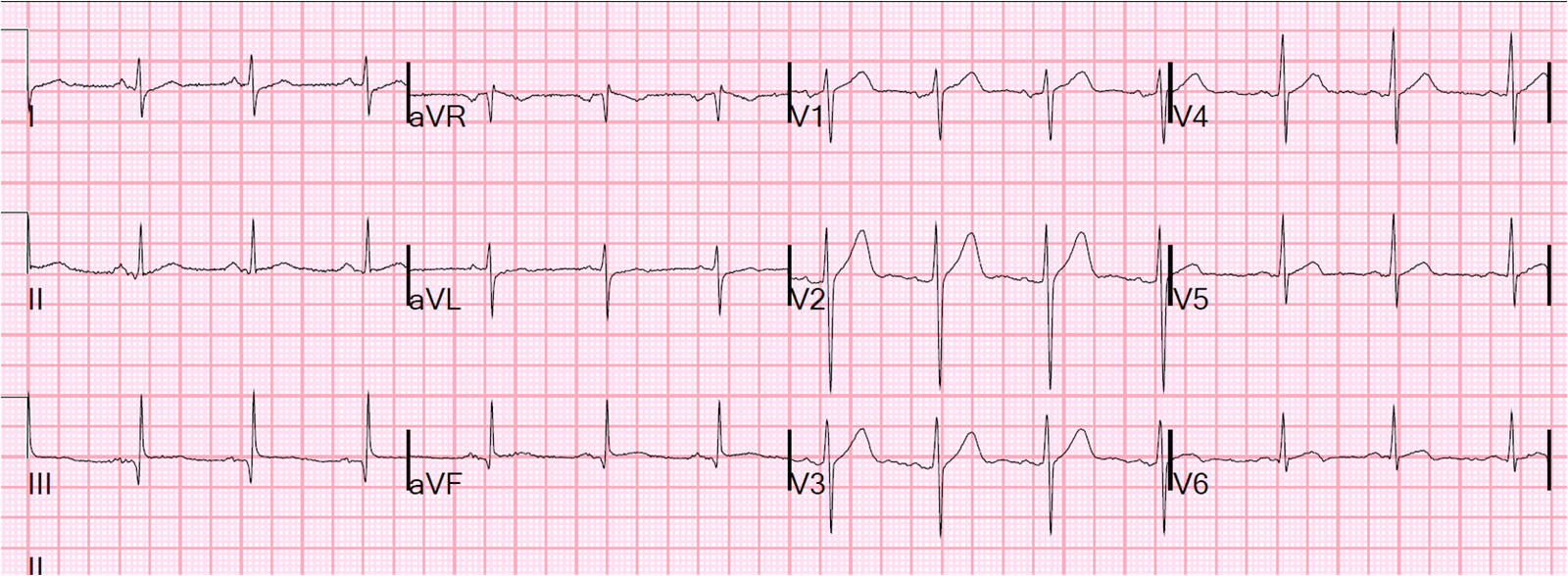
The ECG from the clinic was sought for comparison:
 |
| Compared to this one, the ST depression in I and aVL seen above is new and T-waves are nonspecifically different in diffuse leads. |
The patient continued to have chest pain of an ischemic quality. The clinical presentation worried the ED physicians, so they performed a bedside ultrasound (parasternal short axis view):
Cardiac Ultrasound Parasternal Short Axis from Stephen Smith on Vimeo.
 |
| The curved white line shows the wall (lateral) which has hypokinesis. Note that the hypokinetic area is full thickness, not thinned out as in old MI. Therefore, it is consistent with acute infarct. |
The wall motion abnormality confirms that these nonspecific T-wave changes are indeed ischemic. The chest pain is therefore ischemic. The physicians attempted to control the pain with nitroglycerine, both sublingual and intravenous, titrating to 60 mcg/min, and BP down to 100/57. Thus, they were trying to treat this “NonSTEMI” medically, as there was no ECG indication for immediate reperfusion therapy.
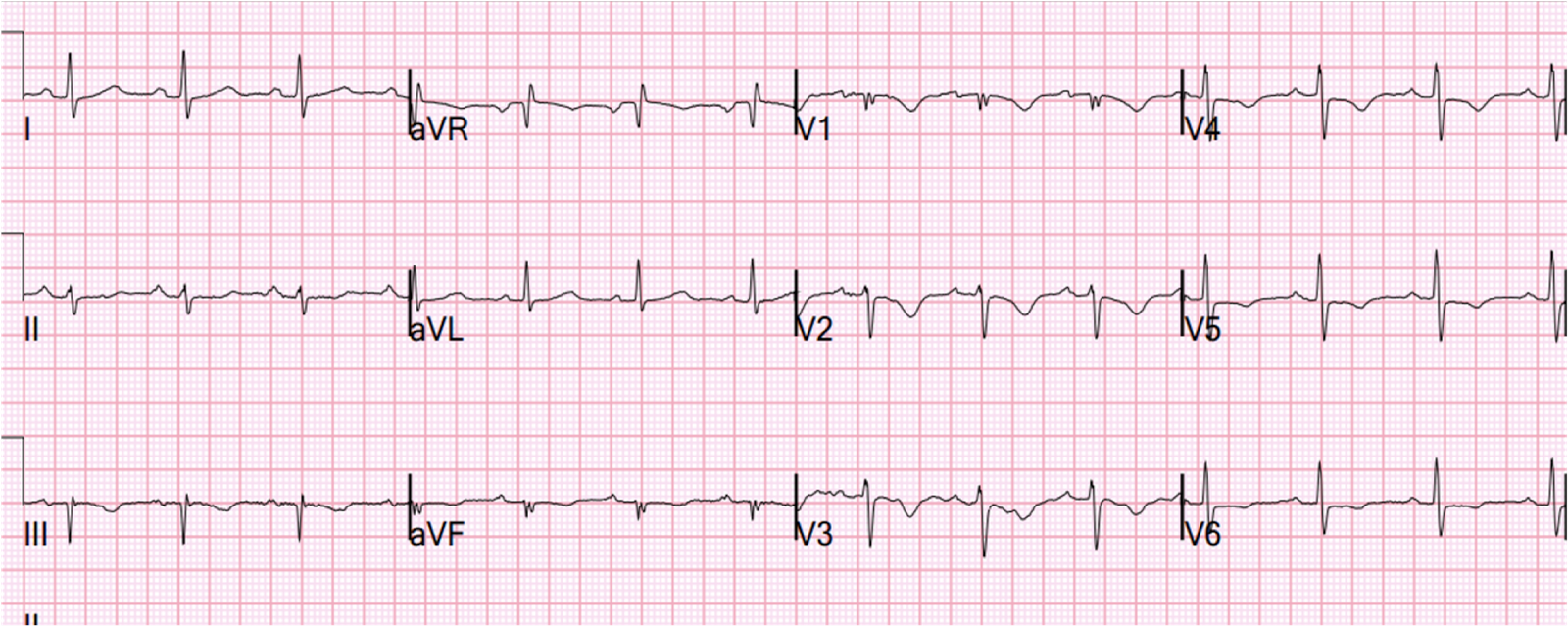
They recorded a posterior ECG:
 |
| Leads “V4” to “V6” are really V7 to V9. Note the low voltage of posterior QRS because of more distance from the heart and because of air (lung) between heart and ECG leads. Thus, only 0.5 mm in 1 lead is considered posterior STEMI. Here there is no ST elevation. However, leads V2 and V3 are the same as the first ECG and the T-waves show are not very different. Thus, the patient has dynamic T-waves. |
The echo and dynamic T-waves confirm ACS. Definite ischemic pain which is refractory to medical therapy is an indication for reperfusion therapy. It is important to remember that approximately one third of NonSTEMI have an occluded infarct related artery at cath.
Heparin and Clopidogrel were given and the patient was taken to cath (after which the first troponin returned slightly elevated). He was found to have severe LAD disease and an occluded 1st Obtuse Marginal off the circumflex. This was opened and stented. The troponin I (Ortho Clinical Diagnostics) peaked at 45.8 ng/ml (quite high). Formal echo later showed anterolateral hypokinesis and an EF of 55%.
The artery was occluded and the myocardial territory at risk was very significant, yet the ECG did not have diagnostic ST elevation. This is common. Fantastic management led to rapid therapy and salvage of significant myocardium.