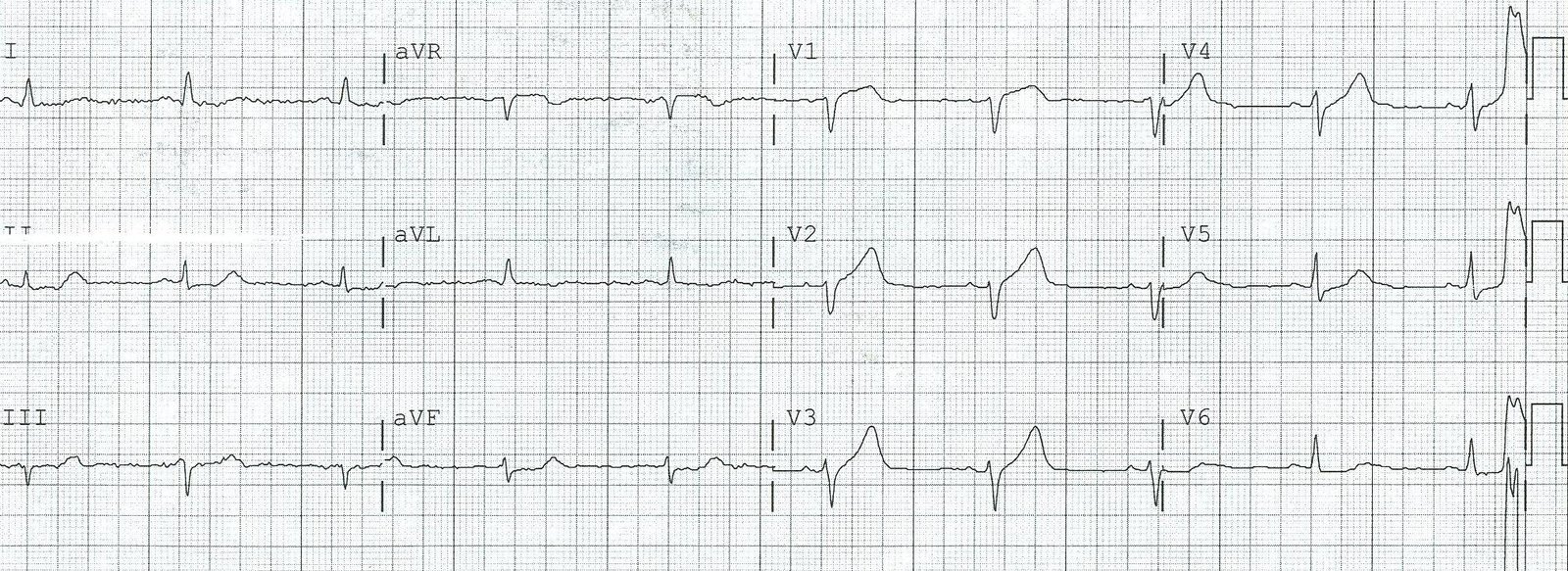
A 40-something yo woman with several coronary risks but no history of coronary disease developed 10/10 “gnawing” retrosternal chest pressure at rest at 7:30 PM. She thought it was reflux, but antacids did not relieve it. She did not arrive in the ED until she had had pain all night (not certain if it was constant or intermittent). Here is her ECG that next AM:
 |
|
|
Let’s look at the limb leads enlarged:
 |
|
|
This is very suspicious for inferior MI of unknown age. It could be old MI with persistent ST elevation, or it could be subacute MI with new Q-wave, but is unlikely to be very acute (with a Q-wave and without large T-waves). If it is a subacute MI, there should be a positive troponin.
The first troponin I returned at 0.74 ng/ml, diagnostic of acute MI. Is this STEMI or NonSTEMI? That is an arbitrary definition, based on millimeters of ST elevation. Every physician should know that biologicial systems do not follow millimeter rules, so many “NonSTEMIs” are due to coronary occlusion.
The important thing is whether the patient has ongoing ischemia after almost 12 hours of chest pain, and as long as the ST segments are elevated or depressed, or the patient has chest pain, one must assume there is ongoing ischemia and do something about it. She did receive antithrombotic and antiplatelet therapy, and nitroglycerine, but her pain did not subside until she received hydromorphone. Then it was not until a second troponin returned at 4.40 ng/ml 4 hours later, that she was taken to the cath lab.
Cath revealed a 100% occlusion of the mid- first obtuse marginal (OM-1). Troponin I peaked at 49 ng/ml. Echo showed an inferolateral wall motion abnormality and concentric hypertrophy.
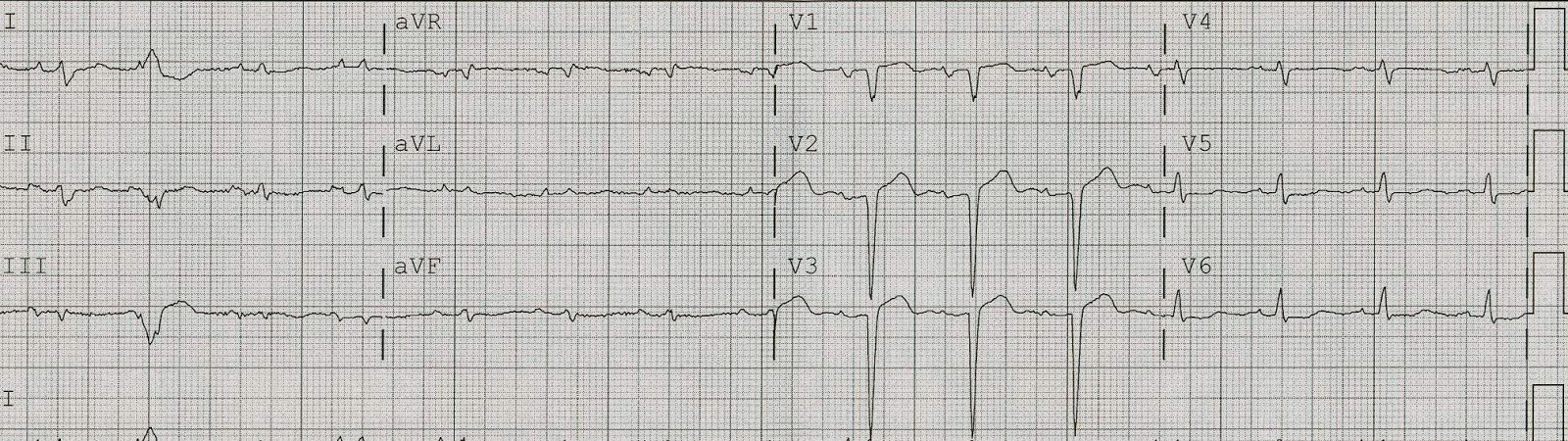
Here is her post cath ECG for comparison:
 |
|
|
Here it is enlarged:

Learning points:
1. Any ST depression in aVL is abnormal. We studied consecutive inferior STEMI patients and 100% (154 of 154) had some ST depression in aVL; among pericarditis controls, zero of 49 had any ST depression). What we don’t no for certain is how many inferior early repol cases have some ST depression in aVL, but it is, in my experience, exceedingly rare, and this case does NOT qualify for early repolarization, which must have good R-wave amplitude in all of II, III, and aVF (here there is a Q-wave in III).
On occasion ST depression in aVL may lead you stray, as in this recent post (which is an anomoly).
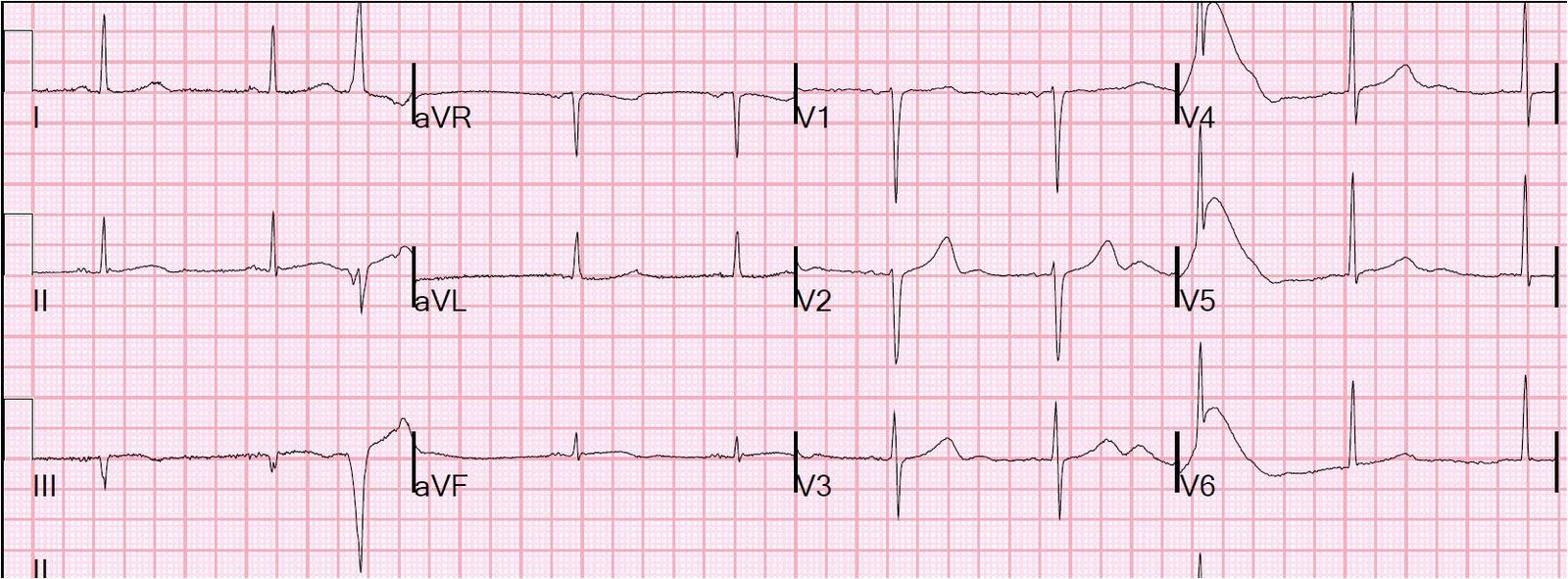
Here is an example of inferior (and lateral) ST elevation due to early repolarization:
 |
| Notice there is 1. Excellent R-wave amplitude, 2. No ST depression in aVL, 3. Proportional T-waves. There is also 4. a short computerized QTc (in this case very short at 354 ms). Notice there is also 5. normal atrial repolarization wave (PR depression); this is not a case of pericarditis! |
2. “NonSTEMIs” may be large and due to complete persistent coronary occlusion that needs emergent reperfusion. Millimeters do not measure occlusion. Large MI may be very subtle on the ECG. This was not a small MI, with peak troponin I of 49.0 ng/mL (large MI).
3. Inferior MI does not always mean Acute MI. This patients initial ECG could represent old MI with persistent ST elevation, subacute MI, or old MI with superimposed acute MI. When the patient has such typical pain, and especially when you have a positive troponin, assume it is acute or subacute. With such a minimal troponin elevation, this was NOT subacute. As it turned out, the myocardium had been ischemic, with only minimal infarct, during those 12 hours, as evidenced by the only minimally elevated troponin.
4. Opiates will obscure the diagnosis of MI. Morphine has been associated with higher mortality in ACS and this is at least partly because the relief of pain is confused by physicians as relief of ischemia. There may even be other mechanisms.
5. If in doubt, get an immediate echocardiogram. In this case, it would have confirmed MI and allowed for earlier cath lab activation. It may not differentiate old MI from acute MI, but absence of WMA would be helpful in finding a false positive. However, they can produce false negative results even in very large MI!
6. Positive troponins alone are not grounds for cath lab activation. There must also be ongoing ischemia as evidenced by either the ECG or ongoing pain, both of which were positive in this case.