A 24 yo with no past medical history and no risk factors except for tobacco smoking presented with chest pain. The pain started in her left chest at 6:20 AM and radiated up through her arms and into her back. She admitted to drinking heavily the previous night and returned home about 1:30 or 2 AM. She had multiple episodes of vomiting overnight. She’s never had chest pain like this before. BP was 140/100 and pulse of 93. There was no rub on exam.
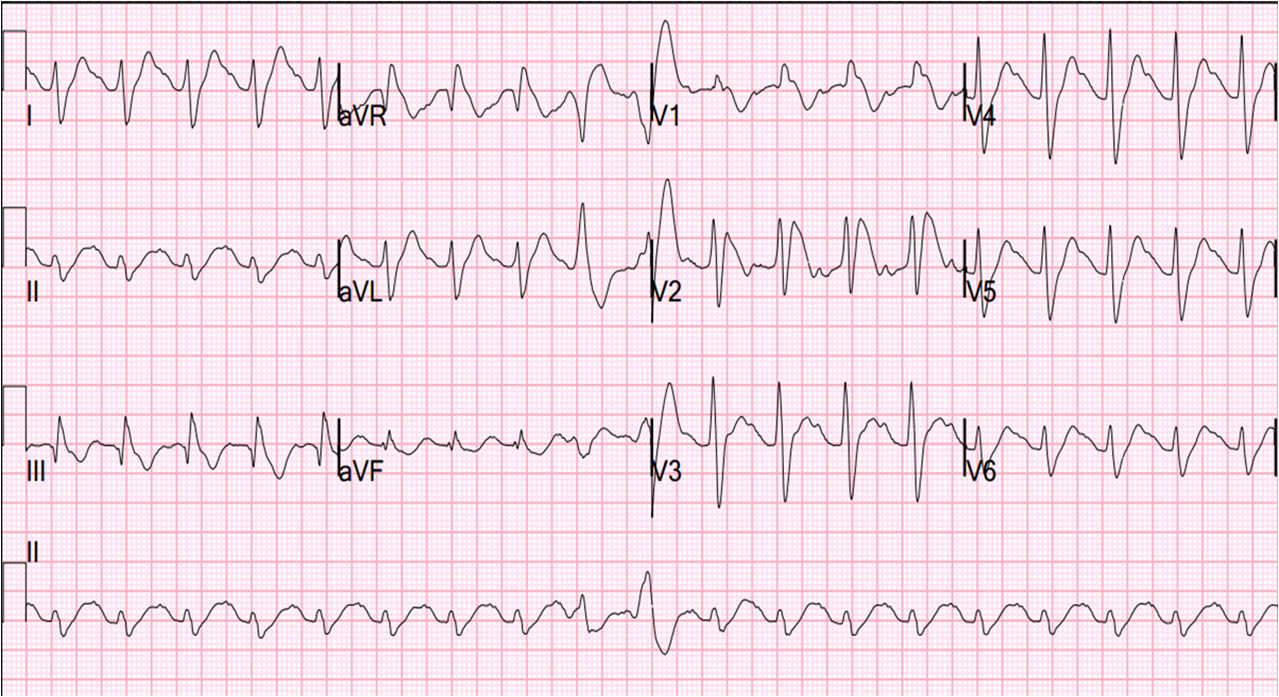
Here is her prehospital ECG at 0720:
 |
|
|
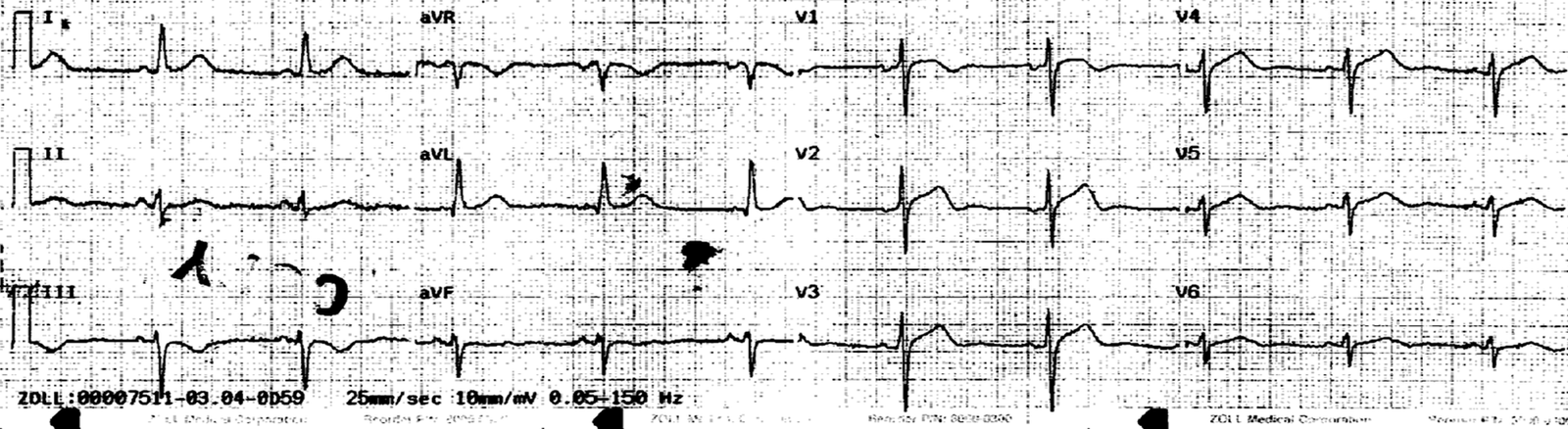
She was given 2 sublingual NTG and her pain improved from 10/10 to 7/10, and continued to improve. Here is her first ED ECG at 0748:
 |
|
|
Chest X-ray confirmed absence of Boerhaave’s syndrome.
Some might suspect pericarditis in a young person with diffuse ST elevation. However, you diagnose pericarditis at your peril! I believe pericarditis is over diagnosed, even in the literature, and that many cases assumed to be pericarditis in the past would not be proved to be Acute MI. This is conjecture based on many cases that I have seen, not based on peer-reviewed evidence.
Furthermore, in our study of benign inferior ST elevation vs. inferior STEMI, ST depression in aVL was nearly perfect in diagnosing MI.
I activated the cath lab immediately.
3 cardiologist came to the ED and opined that this was pericarditis. I told them that with STD in aVL it is acute MI until proven otherwise.
They insisted on doing an echo first. A bedside echo performed by a world expert, Dr. Richard Asinger, showed no effusion, and he could not discern a wall motion abnormality. The patients pain was almost gone by this time.
While waiting for the team, we recorded another ECG at 0826:
 |
|
|
And a right sided ECG at 0827:
 |
|
|
At cath, the culprit was a proximal LAD lesion (open, with TIMI-3 flow)! It had embolized to the distal LAD, which was a “type III” or “wraparound” LAD supplying the inferor wall. So this was an antero-infero-lateral MI. The proximal lesion was stented and the distal was treated with antiplatelet and antithrombotic therapy.
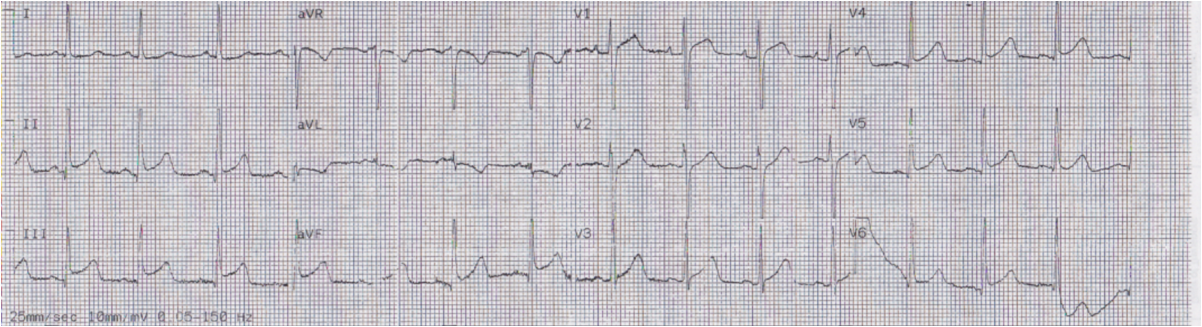
The next day she has reperfusion T-waves in the anterior leads, as well as inferior and lateral leads:
 |
|
|
Formal Echo later showed moderate hypokinesis of the septum and dense hypokinesis of the apex and inferior wall. Peak troponin I was 24 ng/ml.
We always look for explanations when young people have MI. “They must have done cocaine.” “They must have high cholesterol.” But sometimes coronary atherosclerosis is accelerated, or there is one focal lesion, without good reason. Her lipids were: LDL 139, VLDL 10, HDL 70, total cholesterol 219.
Lessons:
1) Myocardial Infarction does occur in young women! They need not have a lot of risk factors or take cocaine. In young women with STEMI, the diagnosis is more often missed or delayed than in any other demographic group, probably because of the bias that leads us to say, as my chief of EM always expresses it: “Nah, couldn’t be.” MI is much more common in young people, including women, than previously recognized. Many MI in very young women may be due to spontaneous coronary dissection, but this is not the most common etiology. If the ECG is diagnostic, as in this case, believe it! Do not try to convince yourself that it “couldn’t be.”
There was an important article published in fall of 2012 showing that young women with STEMI have longer Door to Balloon times and higher mortality. There are a couple smaller studies with the same findings here and here.
2) You diagnose pericarditis at your peril
3) Absence of Wall motion abnormality may be misleading, especially if the pain and/or ECG abnormalities have resolved. In this case, the difference between the informal and formal echo was the use of Definity contrast.