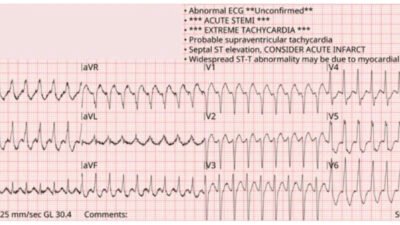
A man in his 60s was found down in the park. Bystanders initiated CPR, but when EMS arrived he had a pulse and it was not clear that he had actually arrested at all. He received naloxone with “some improvement” reported. He had unidentified pills in his pocket. His ECG is shown.
ECG 1

What do you think?
I sent this to the EKG Nerdz. Dr. Smith and Dr. Hellerman immediately replied that they thought it was “fake“. (This means they thought it was not an OMI, but rather an ECG that mimics OMI and could fool non-experts.)
I sent it to a separate group of friends called “OMI Royals” (loyal subjects of the PMCardio Queen of Hearts AI model).
Arron Pearce said it did not look ischemic — “The T waves anteriorly have a nice curve up to a pointed peak.” Nanashī acknowledged that although he recognized it as a mimic, it would be hard to explain why to a novice OMI interpreter. Dr. Floyd noted that the “T wave morphology just doesn’t look concerning.” Dr. Ghali dispensed with it simply — “Looks fake to me.”
See also this post: Quiz post: do either or both of these patients have high lateral OMI / South African flag sign?
What do all these ECG interpreters have in common? Answer: They are all blog readers who have engaged in deliberate practice, constantly quizzing themselves and one another to refine their pattern recognition. But none of us can learn as many patterns as quickly and permanently as the Queen of Hearts.
The Queen saw no OMI. The model output was 0.23. It takes a score of 0.50 or higher to register as positive. Below 0.30 is very low and would be extremely unlikely to be OMI.
New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/
Compare that to the following ECG from a different patient which shows OMI:
ECG 2

Here are the limb leads side by side. In each pair, the left side shows ECG 1 (not OMI), and the right side shows ECG 2 (OMI). Try to focus on the subtle differences:
Limb Leads

Comparing them, we see that ECG 1 has the following features:
- The T waves are very asymmetric (slow upslope, rapid downslope), and the area under the curve is small relative to the QRS amplitude
- The terminal QRS slurs into the ST segment smoothly
- The ST takeoff is slow and concave
- The voltage tends to be much higher
By contrast, ECG 2 shows:
- More symmetric T waves with larger volume relative to the QRS
- The terminal QRS has a very abrupt, almost angular takeoff into the ST
- The ST is less concave, more flat
- The voltage is lower
And the precordial leads:
Precordial Leads

The changes we see here are similar to what the limb leads showed, but the differences in T waves are more pronounced.
Back to the case:
The patient was activated as a STEMI and taken for emergent angiography, which showed mild coronary artery disease (including intravascular ultrasound of the LAD to avoid missing plaque rupture with spontaneous recanalization, credit for completeness). Four serial high sensitivity troponin I measurements over the course of five hours were all within normal limits. Echocardiogram showed normal left ventricular size, normal left ventricular ejection fraction, normal wall motion, and concentric remodeling (structural geometric change in the absence of hypertrophy).
When I discussed this case with cardiology colleagues, they felt there was no way to justify avoidance of cath lab activation given the impressive ST elevation (STEMI positive!) on the ECG.
I would say it is entirely reasonable to manage this patient without immediate angiography, especially given that the pre-test probability for OMI was very low to begin with. In fact, the ER note specifically documents that the patient “denies any pain or complaints on arrival.” Low pre-test probability for OMI plus an ECG that shows no evidence for OMI.
So, what does the ECG show? Normal variant ST elevation. Repeat tracing in the ER is shown below:

The pattern is still present, but more subtle now. It is an unfortunate and frustrating fact that neither dynamic change nor reciprocal change are specific for OMI, and both were present here!
Learning points:
- Even ST elevation with reciprocal change is not necessarily specific for ischemia
- Normal variant ST elevation can be quite impressive and satisfy STEMI criteria
- Emergency ECG triage is going to continue to improve as access to Queen of Hearts increases
- Normal Variant STE sometimes has reciprocal ST depression. When it is inferior STE, there is sometimes reciprocal STD in aVL. So the presence of reciprocal STD, by itself, is not confirmatory for OMI.
= =
======================================
MY Comment, by KEN GRAUER, MD (9/19/2025):
I love cases like today’s — in which a group of my esteemed EKG Nerdz colleagues render their objective opinions on challenging ECGs. I view “the Answer” regarding the interpretation of today’s initial ECG as consisting of 2 Parts: i) Whether this initial ECG indicates an acute OMI that merits immediate cath lab activation?; and, ii) How best to proceed clinically?
= = =
My Thoughts:
I agree with my EKG Nerdz colleagues — that today’s initial ECG looks more like a repolarization variant than an acute OMI. That said — I was not completely certain of this initial impression.
- I would not have activated the cath lab on the basis of the history we are given and the initial ECG in today’s case.
- That said — I was not 100% certain of this impression. As a result — I would have gotten more information, some follow-up tracings, and a minimum of 2 Troponins before I’d be comfortable that an acute event was completely ruled out.
= = =
Today’s Initial ECG:
To facilitate comparison of the 2 ECGs done in today’s case — I’ve put them together in Figure-1. To emphasize, that although there are a number of descriptive findings in today’s initial ECG that should be noted — Clinical correlation gave me the impression that today’s initial tracing was probably a “fake”. For completeness — I specify my thought process as follows:
- The rhythm in ECG #1 is sinus at ~80/minute. But note that there is 1st-degree AV block (ie, PR interval = 0.24 second) — so not completely “normal”. By itself, 1st-degree AV block is not necessarily a worrisome finding — but its presence here should raise awareness.
- The most remarkable finding in ECG #1 is the ST elevation in high-lateral leads I and aVL. Although the amount of ST elevation is a bit more than usually seen with repolarization variants — the shape of the ST elevation is with an upward concavity (ie, “smiley”-configuration) that is more commonly associated with repolarization variants.
- There is ST-T wave depression in lead III — that might be interpreted as a “reciprocal” change to the ST elevation seen in oppositely-directed lead aVL. That said — when the QRS complex is predominantly negative (as it is in lead III) — the ST-T wave depression that we see in lead III is not necessarily an ischemic change (because the T wave axis in the limb leads normally follows fairly close behind the QRS axis).
- Elsewhere in the limb leads of ECG #1 — there is subtle flattening of the ST segment in lead II — and of the ST-T wave in lead aVF — but these findings are nonspecific.
- Finally — lead aVF is fragmented (ie, the notching within the dotted RED oval in this lead). While fragmentation may be an indication of “scar” — isolated to lead aVF, it is a nonspecific finding.
In the chest leads of the initial ECG:
- IF the concern from the limb leads was the ST elevation in high-lateral leads I and aVL — then I would expect to see some indication of acute posterior involvement. This is entirely absent. Instead of the ST segment flattening (if not depression) in leads V2,V3 that we’d expect with posterior involvement — there are instead upsloping ST segments in these leads, with some ST elevation in lead V2.
- The QS in leads V1,V2 is nondiagnostic.
- Slanted BLUE lines in leads V3-thru-V6 highlight tiny q waves that are usually not seen as far over as in lead V3. That said — ample R wave amplitude takes over beginning in lead V4, such that these tiny q waves are non-diagnostic.
- KEY Point: The above ECG findings in today’s initial tracing are seen in a 60s man who was “found down” in the park without any confirmation that cardiac arrest had occurred. And, this patient was asymptomatic without chest pain on arrival in the ED. Rather than concave-up ST elevation — if ECG #1 represented an acute OMI, I would have expected a more worrisome appearance of the ST elevation in these lateral leads and/or suggestion of some reperfusion T waves in this man who was “down”, but who is now apparently asymptomatic!
- BOTTOM Line: Given the history, this patient will be admitted to the hospital. This means that he can be closely observed! Therefore — I don’t see the need to rush to the cath lab given asymptomatic status in association with this nondiagnostic initial tracing. I’d expect Troponins and repeat ECGs to clarify the diagnosis in timely fashion.
= = =
Figure-1: Comparison of the 2 ECGs in today’s patient.

= = =
What About the Repeat ECG?
Surprisingly — the repeat ECG in Figure-2 does show a number of changes compared to the initial ECG.
- Sinus rhythm is again present — at a slightly faster rate than was seen in ECG #1.
- The relative amount of ST elevation in lateral leads I and aVL is less in the repeat ECG compared to the initial tracing. Similarly — the relative amount of ST-T wave depression in lead III is also less.
- The nonspecific ST-T wave flattening in leads II and aVF remains.
- The fragmentation in lead aVF is no longer present (Perhaps this is a result of the slight change in frontal plane axis).
- Apart from slightly earlier transition in the chest leads — the QS in leads V1,V2 with slight ST elevation in V2 and tiny q waves in leads V3-thru-V6 remains.
- What is new — is upward sloping ST elevation with J-point notching (BLUE arrows) in leads V4,V5,V6.
- BOTTOM Line: One might be tempted to interpret the above ST-T wave changes between ECG #1 and ECG #2 as a “dynamic” change. Instead — I thought the overall appearance in the repeat ECG in leads I,aVL; III; and in the chest leads (especially with the J-point notching) is much more suggestive of a repolarization variant (and not of an acute evolving event).
- Multiple serial hs-Troponin levels were all normal — which given the lack of chest pain, would confirm for me that there is no acute OMI.
- Learning Point: On occasion — benign repolarization variants may manifest some change in ST-T wave morphology on serial repeat ECGs, just as we see in Figure-1 (See My Comment in the June 30, 2023 post in Dr. Smith’s ECG Blog).