This is a case seen by one of my great partners at Hennepin County Medical Center Dept. of Emergency Medicine, Dr. Ashley Strobel, @AStrobelMD.
Case
A patient was found down and was quite ill and in shock. The POCUS of his heart showed very poor contractility.
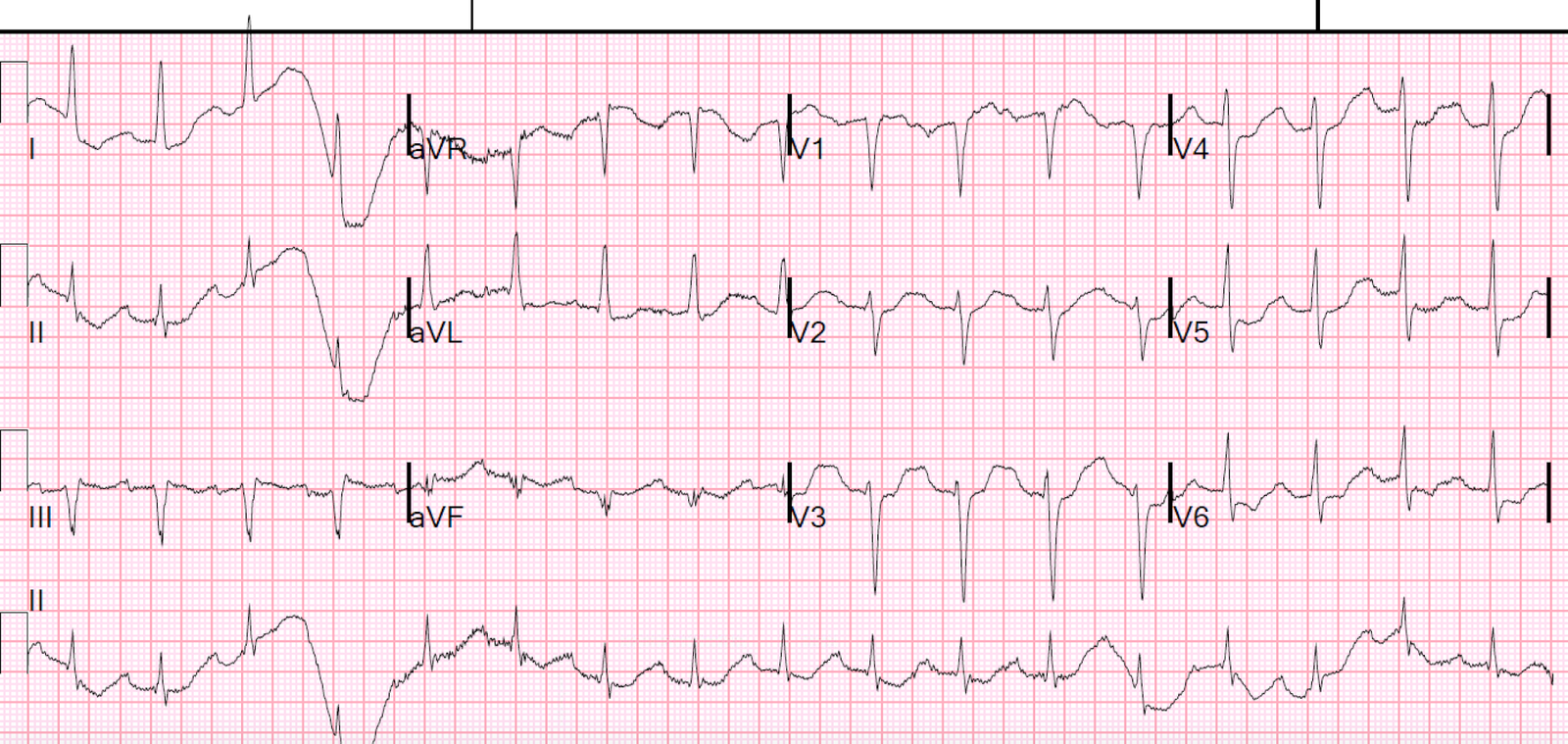
Here is his initial ECG:
 |
| It is a supraventricular rhythm, with grouped beating. What else? |
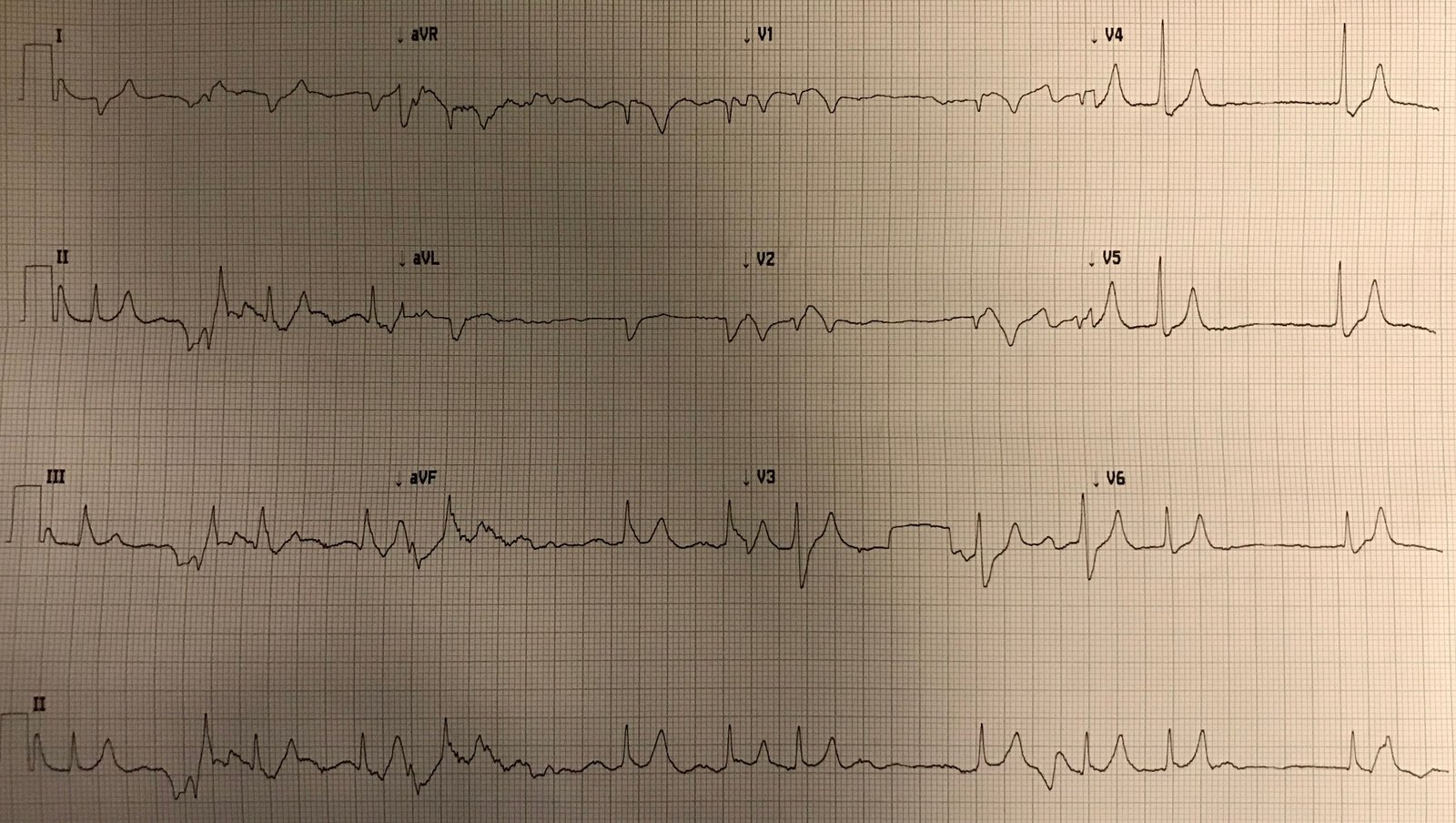
Here is a rhythm strip (10 seconds of all leads):
 |
| Again, there is grouped beating. What else do you see? |
When she showed me this ECG, I was at first distracted by the rhythm, and did not immediately see the life threatening finding. It took me a minute before I looked beyond the rhythm.
What is it?
The QRS is slightly wide, greater than 120 ms. Leads V1 and V2 have domed ST Elevation with T-wave inversion that is very similar to Brugada pattern (“Brugada phenocopy”), similar to my last post.
Brugada pattern should make you think of either hyperkalemia or sodium channel blockade. Additionally, there is T-wave peaking in many leads.
Dr. Strobel suspected hyperkalemia and treated with Calcium and shifting. She was right. The K returned at 7.1 mEq/L.
Here is another post with many cases of Brugada phenocopy due to hyperkalemia:
This ECG is NOT Pathognomonic of Brugada Syndrome
Here are other etiologies of Brugada phenocopy:
http://www.brugadaphenocopy.com/brp-registry.html
Analysis of rhythm
Here is Ken Grauer’s analysis:
“While
there most definitely is a repetitive pattern of group beating (which is a feature of Wenckebach) — this
is NOT completely typical of Wenckebach conduction — because the pause
containing the dropped beat is NOT less than twice the shortest R-R
interval. That’s not to say there can’t be some component of Wenckebach
conduction out of the AV node — but rather to recognize that lack of
this above “footprint” is indeed a bit atypical …. and under normal
circumstances is often a clue that the mechanism may not be Wenckebach
despite group beating …
“That said — T waves
in many leads are tall, peaked and pointed with symmetric upstroke and
downstroke and narrow base in a number of leads in this somewhat widened
QRS rhythm with group beating but no P waves. This strongly suggests
hyperkalemia (which may also be responsible for the Brugada-like V1,V2
findings as well).
“It’s been my experience that
most of the time it is NOT worth one’s while to contemplate arrhythmia
mechanisms when the underlying problem is hyperkalemia — because this
electrolyte abnormality “does not follow the rules” — and because
whatever arrhythmia abnormality we see will “go away” once you fix this
underlying problem of hyperkalemia. Sounds like this is precisely what
happened in your case.”
Learning Point:
Always be on the lookout for hyperkalemia. It comes in many form and can mimic many pathologies.