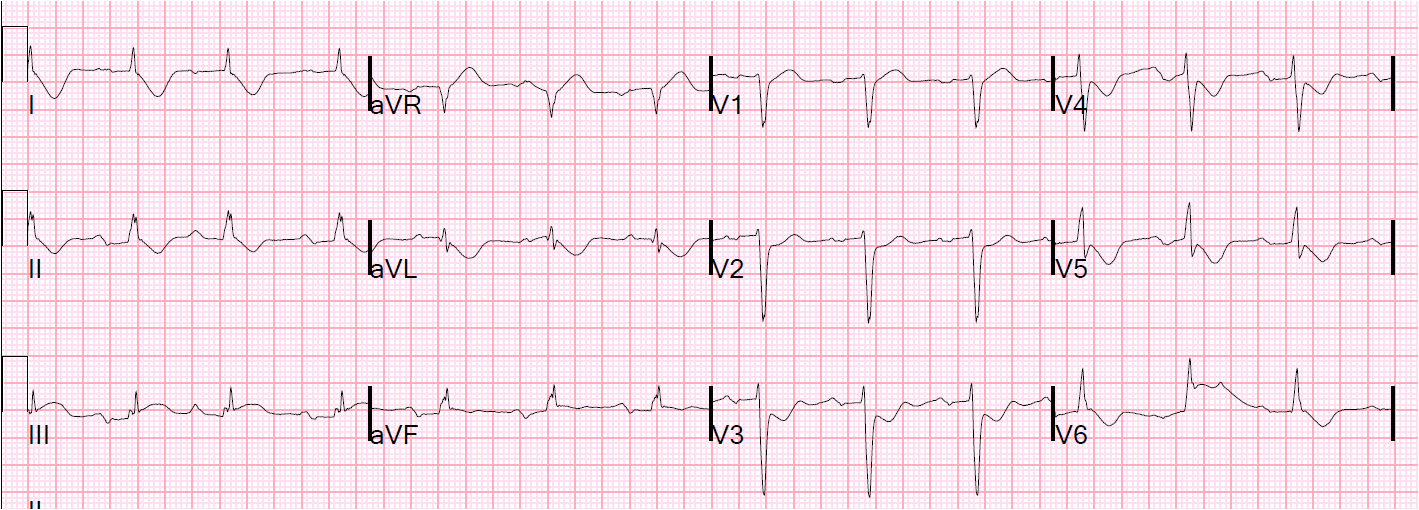
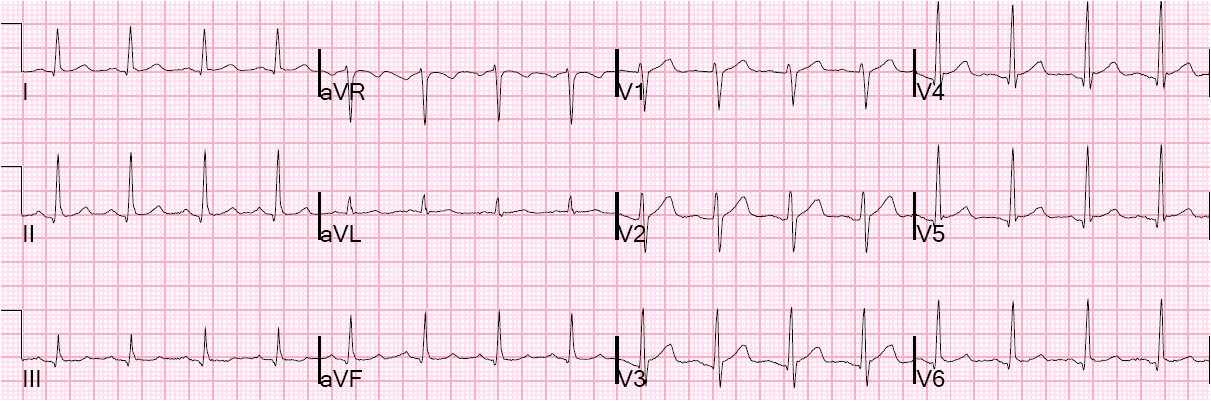
A 32 year old presented with a gunshot wound that seems to have entered the anterior chest with a downward trajectory, traversing his chest wall on the interior, and exiting his left flank. He had anterior chest pain with movement or breathing. An ECG was done as part of the evaluation at 0300:
 |
| There is ST elevation injury pattern in V3-V6, I and aVL, consistent with either myocardial injury or pericardial inflammation. |
ED Echo showed no pericardial effusion and good myocardial contractility and no major wall motion abnormality.
A CT of the chest was done:
 |
| The arrow shows air (in the pericardium?) where the bullet passed directly anterior to the heart. There were no major organ injuries other than diaphragmatic injury and omental hernia |
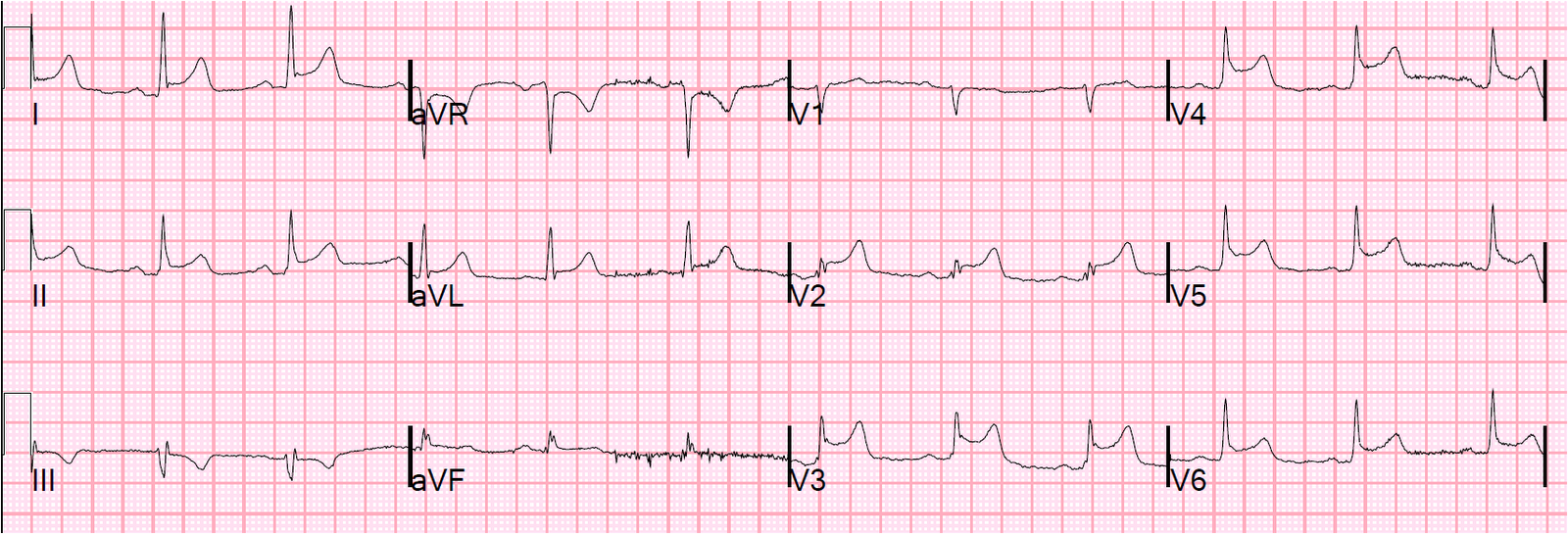
A repeat ECG was done at 0454 (114 minutes later):
 |
| ST elevation is almost entirely resolved |
Troponin I quickly rose to 5.26 ng/ml and an echocardiogram showed a definite, but small, anteroapical wall motion abnormality.
This could be due to direct contusion or to coronary injury, so a CT coronary angiogram was done which showed all coronaries to be patent with no evidence of damage.
The troponin trended down from that peak.
The patient was taken to the OR for repair of a diaphragmatic and omental hernia.
He was discharged on day 4 with no adverse events, including no dysrhythmias.
Diagnosis: myocardial contusion from a bullet