Here is a series of ECGs with increasing ST elevation (STE). They are of a young male with pleuritic, but not positional, chest pain.
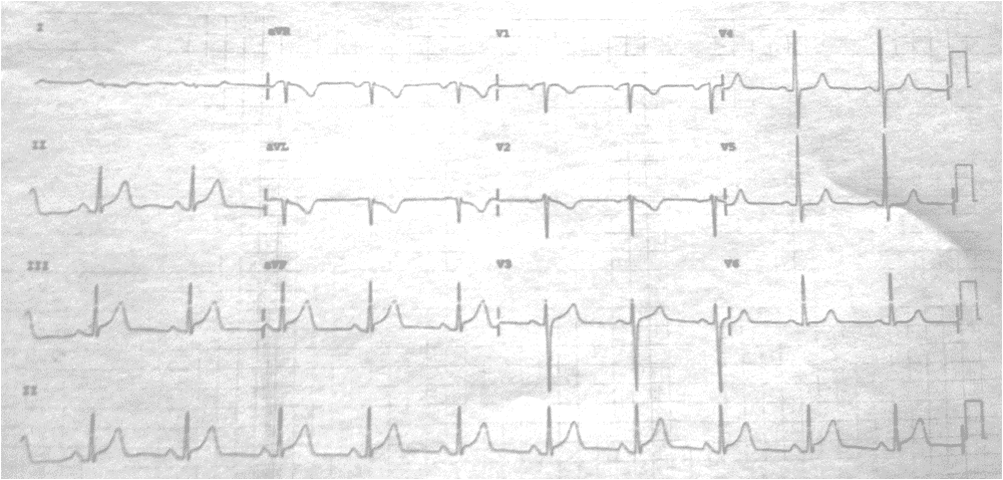
Time zero:
 |
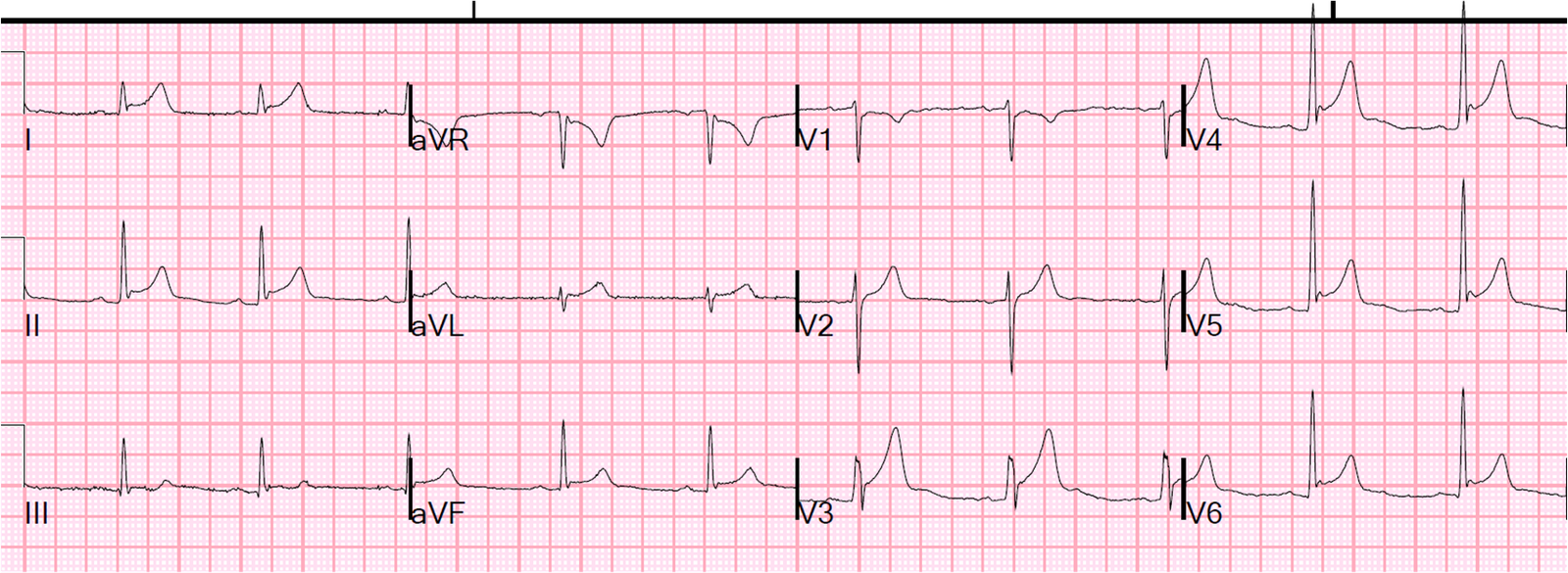
| NSR. No remarkable findings. Minimal STE in V2, V3, and I. QTc 383. LAD occlusion, early repol formula = 18.1 |
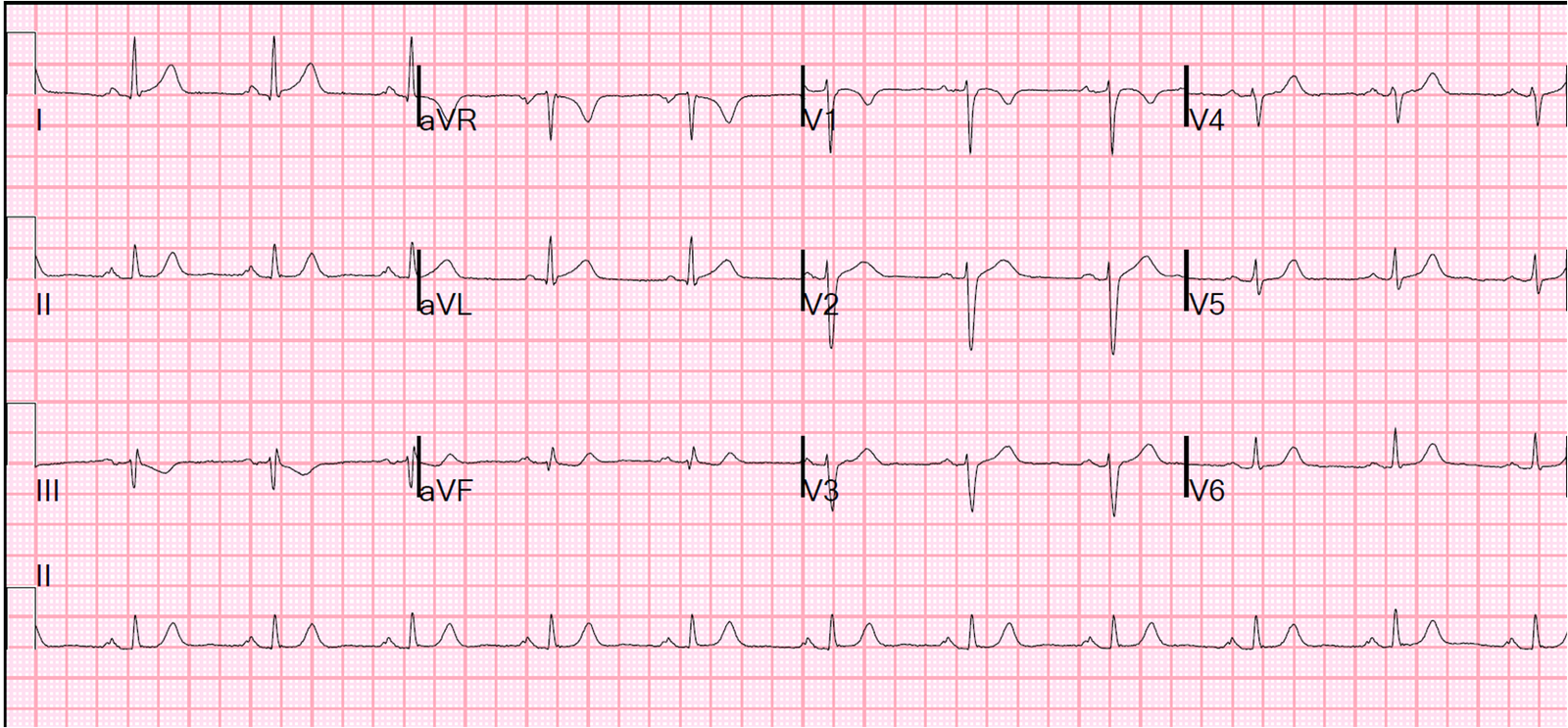
Time = 4.5 hours:
 |
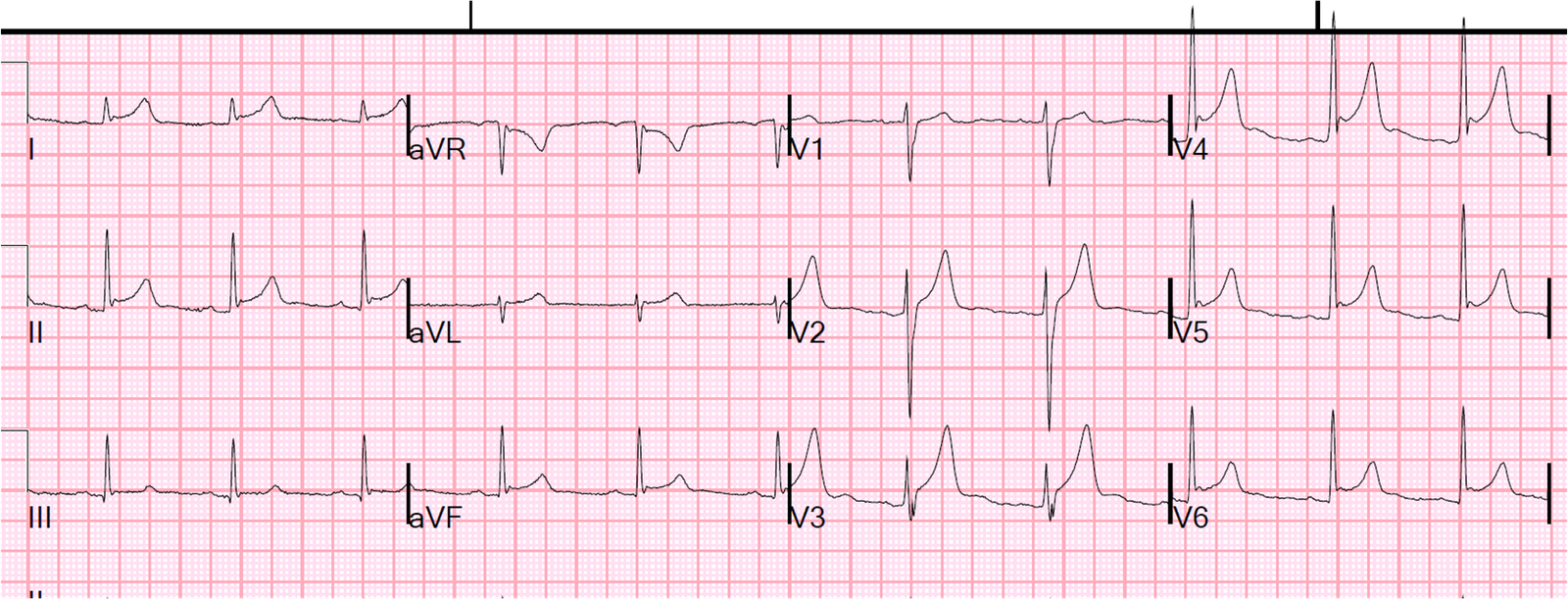
| New, diffuse ST elevation. QTc 384, formula 19.1. The ST axis is about 30 degrees (towards leads I and II, such that there is STE in aVL, I, II, and aVF, but not III) and there is no reciprocal ST depression except in lead aVR). This is very typical for pericarditis or diffuse early repolarization. Pericarditis does not usually have T-wave voltage this high; a high T/ST ratio is more likely to be early repolarization. Additionally, there are very well formed J-waves, typical of early repolarization. It is highly unlikely to be acute STEMI. |
There was no pericardial friction rub and echo revealed no pericardial fluid and no wall motion abnormality, and normal EF.
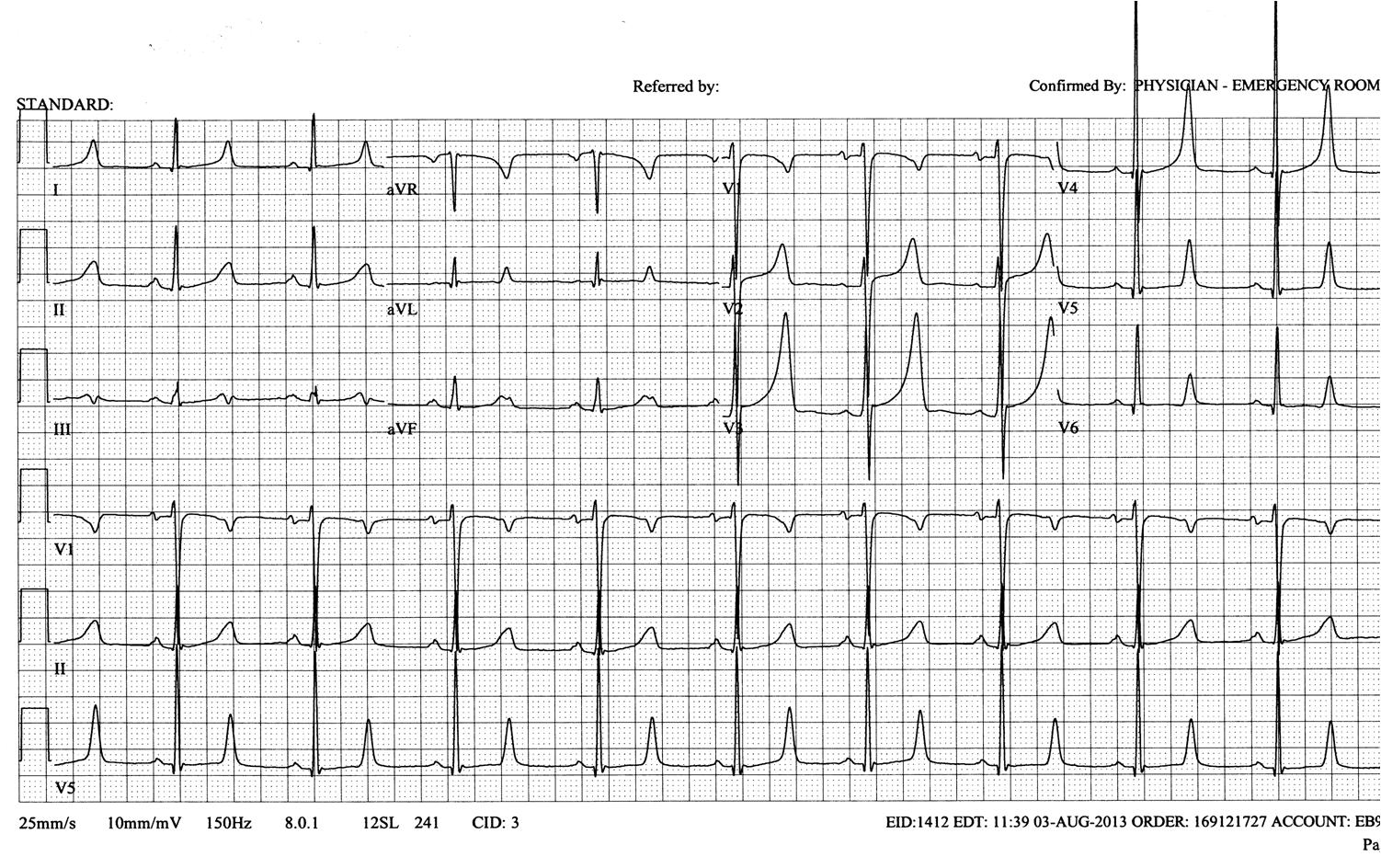
Time = 5.2 hours:
 |
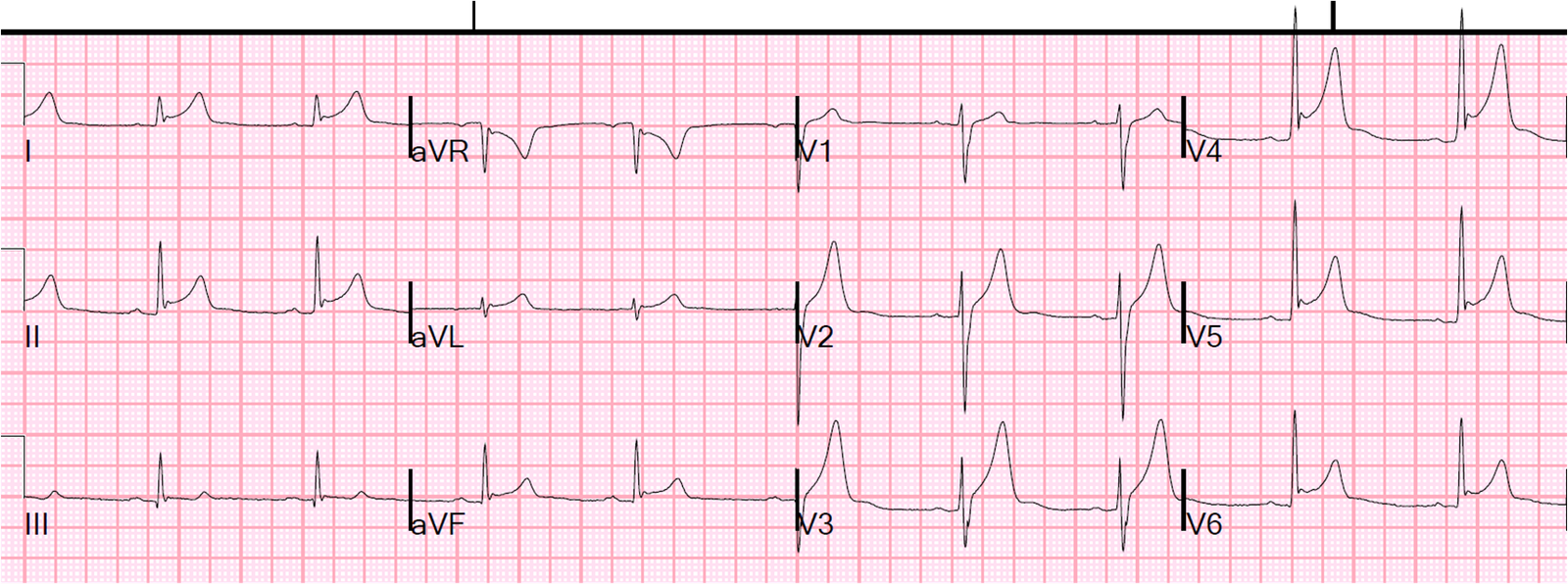
| More ST elevation, especially in lead V2. QTc 389, formula 20.56 |
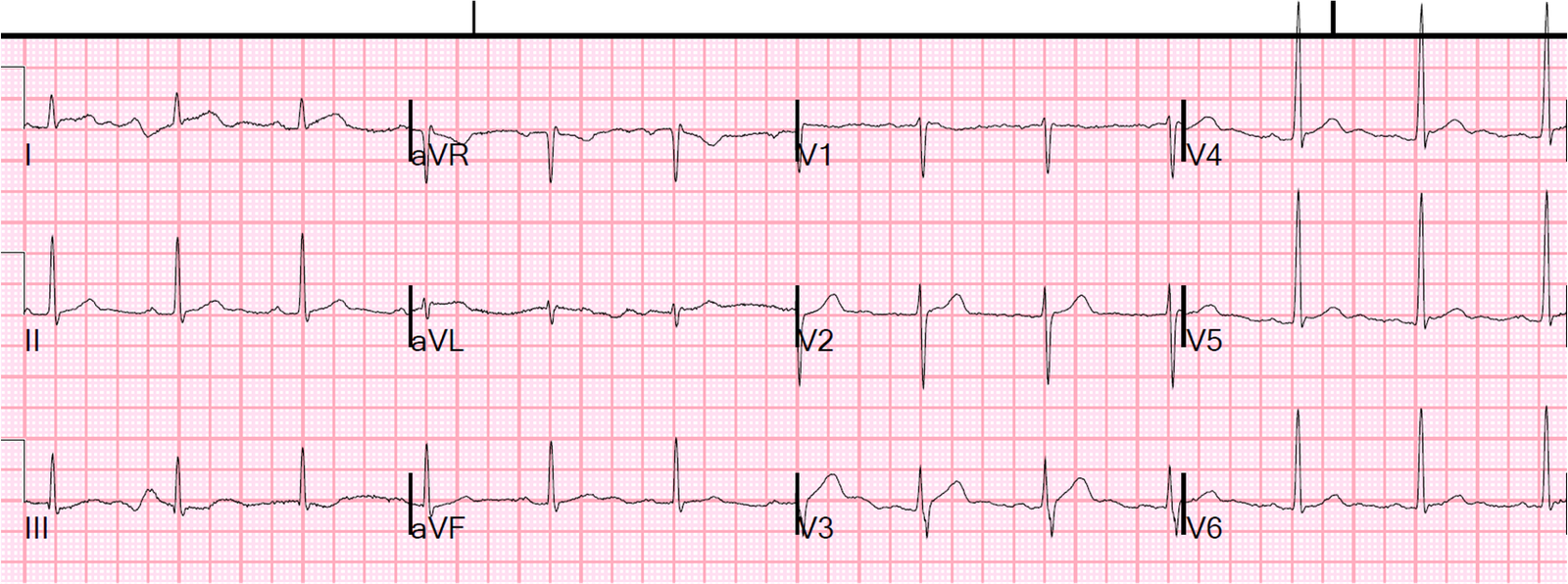
Time = 7.2 hours:
 |
| No change. QTc 389, formula 19.96 |
He ruled out for MI.
Diagnosis: probable dynamic early repolarization. Could it be pericarditis? Yes, but if there is no pericardial effusion and there is good cardiac function with negative troponins (not myocarditis with myocardial dysfunction), then pericarditis would be treated with Nonsteroidal antiinflammatory medications only.
In other words, the really important differential is this: is this STEMI, or is it a more benign etiology? And to make this determination, it is important to know that early repolarization may be dynamic (1, 2). And it may even change from hour to hour, or with heart rate or exercise. We have seen this many times, though it is not common.
The use of the LAD-BER formula may be of great help and lead one to obtain an echocardiogram rather than activating the cath lab.
1. Kambara H, Phillips J. Long-term evaluation of early repolarization
syndrome (normal variant RS-T segment elevation). Am J Cardiol
1976;38(2):157-61.
Kambara, in his longitudinal study
of 65 patients with early repolarization, found that 20 patients had
inferior ST elevation and none of these were without simultaneous
anterior ST elevation. Elevations in inferior leads were less than
0.5mm in 18 of 20 cases. Kambara also found that, in 26% of patients,
the ST elevation disappeared on follow up ECG, and that in 74% the
degree of ST elevation varied on followup ECGs.
2. Mehta MC. Jain AC. Early Repolarization on the Scalar Electrocardiogram. The American Journal of the Medical Sciences 309(6):305-11; June 1995.
Sixty thousand electrocardiograms were analyzed for 5 years. Six hundred
(1%) revealed early repolarization (ER). Features of ER were compared
with race-, age-, and sex-matched controls (93.5% were Caucasians, 77%
were males, 78.3% were younger than 50 years, and only 3.5% were older
than 70). Those with ER had elevated, concave, ST segments in all
electrocardiograms (1-5 mv), which were located most commonly in
precordial leads (73%), with reciprocal ST depression (50%) in aVR, and
notch and slur on R wave (56%). Other results included sinus bradycardia
in 22%, shorter and depressed PR interval in 38%, slightly asymmetrical
T waves in 96.7%, and U waves in 50%. Sixty patients exercised
normalized ST segment and shortened QT interval (83%). In another 60
patients, serial studies for 10 years showed disappearance of ER in 18%,
and was seen intermittently in the rest of the patients. The authors
conclude that in these patients with ER: 1) male preponderance was
found; 2) incidence in Caucasians was as common as in blacks; 3)
patients often were younger than 50 years; 4) sinus bradycardia was the
most common arrhythmia; 5) the PR interval was short and depressed; 6)
the T wave was slightly asymmetrical; 7) exercise normalized ST segment;
8) incidence and degree of ST elevation reduced as age advanced; 9)
possible mechanisms of ER are vagotonia, sympathetic stimulation, early
repolarization of sub-epicardium, and difference in monophasic action
potential observed on the endocardium and epicardium.