A 72 year old male presented in shock. Here is his initial ECG:
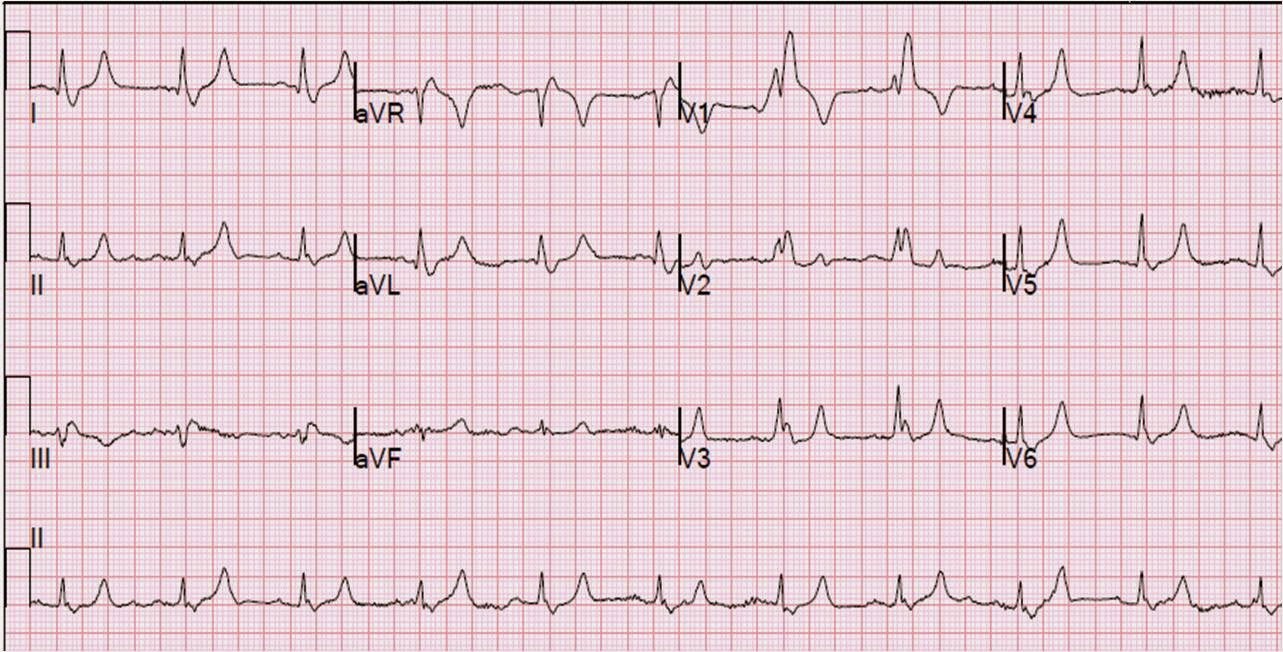 |
| There is a wide complex at 194 ms, with RBBB. Anything else? |
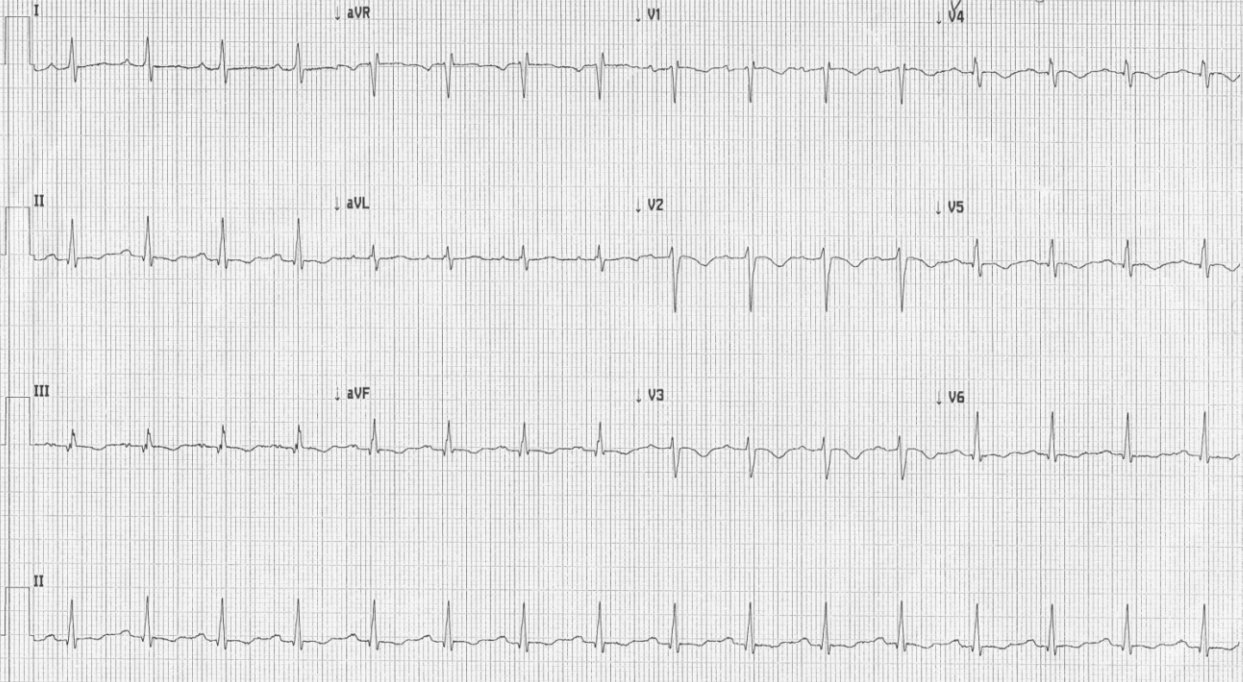
Here is his baseline ECG, also with RBBB:
 |
| There is sinus tach with otherwise normal RBBB; the QRS is 129 ms, average for RBBB. |
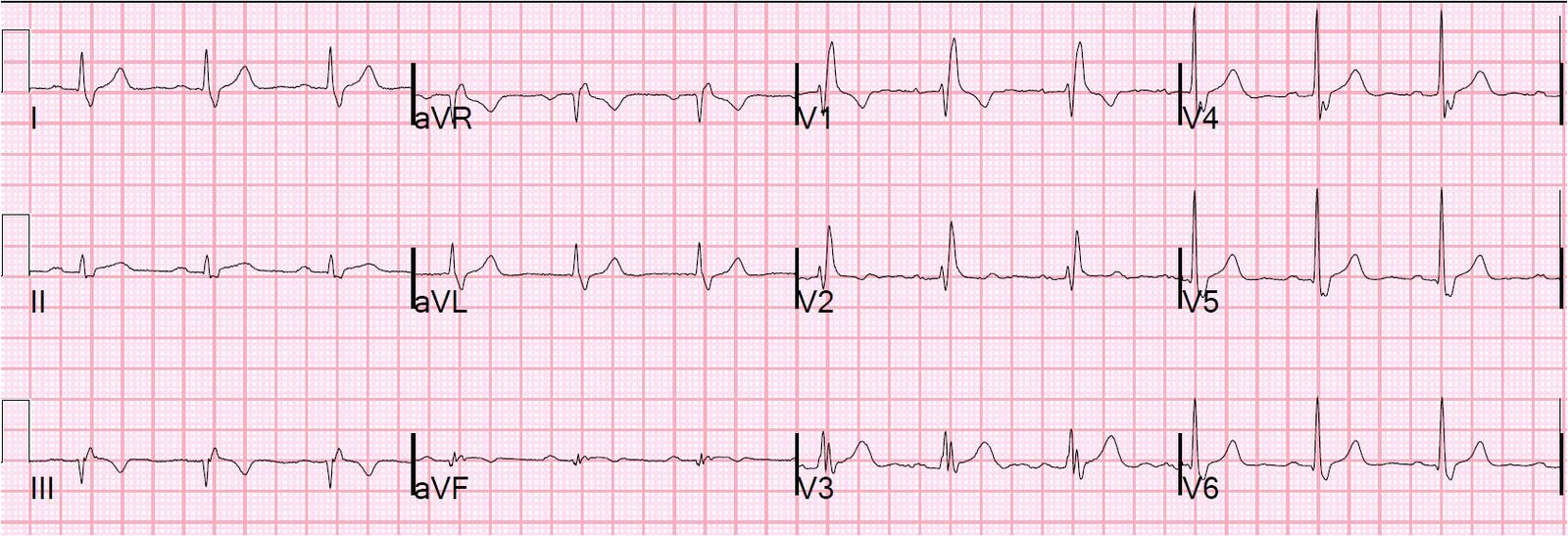
The physicians appropriately recognized that the QRS in the first ECG was far too wide, and that there were peaked T-waves. They immediately administered Calcium, Bicarbonate, D50 and insulin, and repeated the ECG:
 |
|
|
The initial K returned at 7.9 mEq/L, and the repeat K was 5.1 mEq/L (which seems like a rather impossible improvement in a short amount of time, but there is certainly some significant improvement on the ECG).
The patient had urosepsis with renal failure, was resuscitated and dialyzed.
This was recorded the next day, with the K at 3.3 mEq/L:

RBBB by definition has a long QRS (> 120 ms). But very few are > 190 ms. Literature on this is somewhat hard to find, but in this study of patients with RBBB and Acute MI, only 2% of patients with pre-existing RBBB had a QRS duration > 200 ms. This study only reported durations in 10 ms intervals up to 150 ms, but one might extrapolate from it that approximately 10% of patients with baseline RBBB have a QRS duration > 160 ms. 194 ms would be quite unusual.
The point of this is that if you see BBB with a very long QRS, you must suspect hyperkalemia. Then of course the peaked T-waves should tip you off. Unless a patient has severe hypercalcemia (this should be evident by a short QT on the ECG as seen at the bottom of this post), or severe hyperphosphatemia (which is very unusual), treatment with calcium is harmless if you read an ECG falsely positive for hyperkalemia.
So don’t wait for the laboratory K or you might be resuscitating a cardiac arrest (see the case with ECGs #3 and #4 of this post).
How about LBBB, asks one reader?
In this study of consecutive patients with LBBB who were hospitalized and had an echocardiogram, 13% had a QRS duration greater than 170 ms, and only 1% had a duration greater than 190 ms.