This 74 yo male had just returned to his unit bed after successful PTCA of tight lesions of the first diagonal and obtuse marginal coronaries. He complained of chest pain. This ECG was recorded. The previous is below.
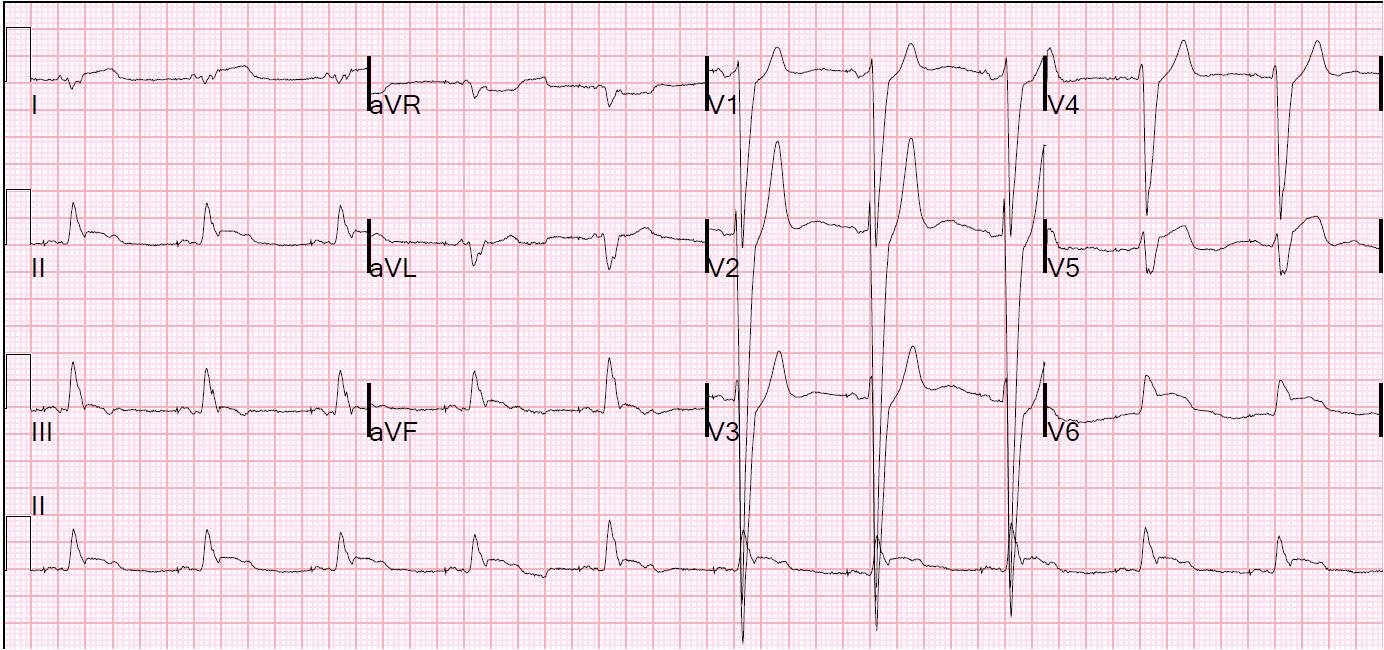 |
| There is LBBB with concordant ST elevation in II and aVF (inferior STEMI) and V6 (lateral STEMI); also concordant ST depression in V2 and V3 (Posterior STEMI). There is also excessively discordant ST elevation in V5 (ST/S ratio 2:5 = 40%; excessive is > 20%). Compare with baseline ECG below. |
 |
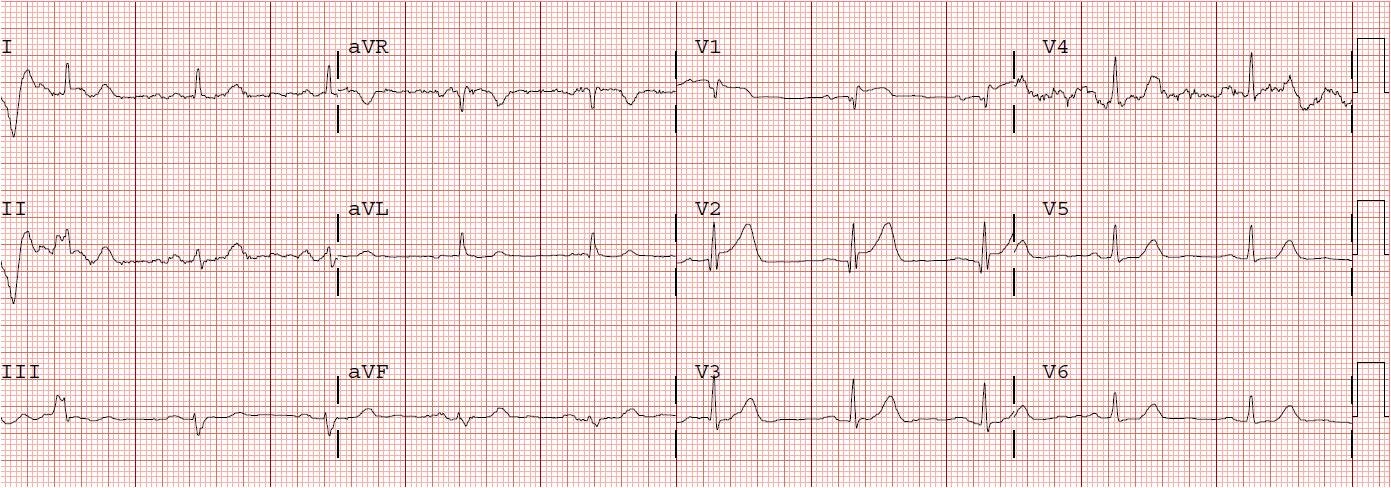
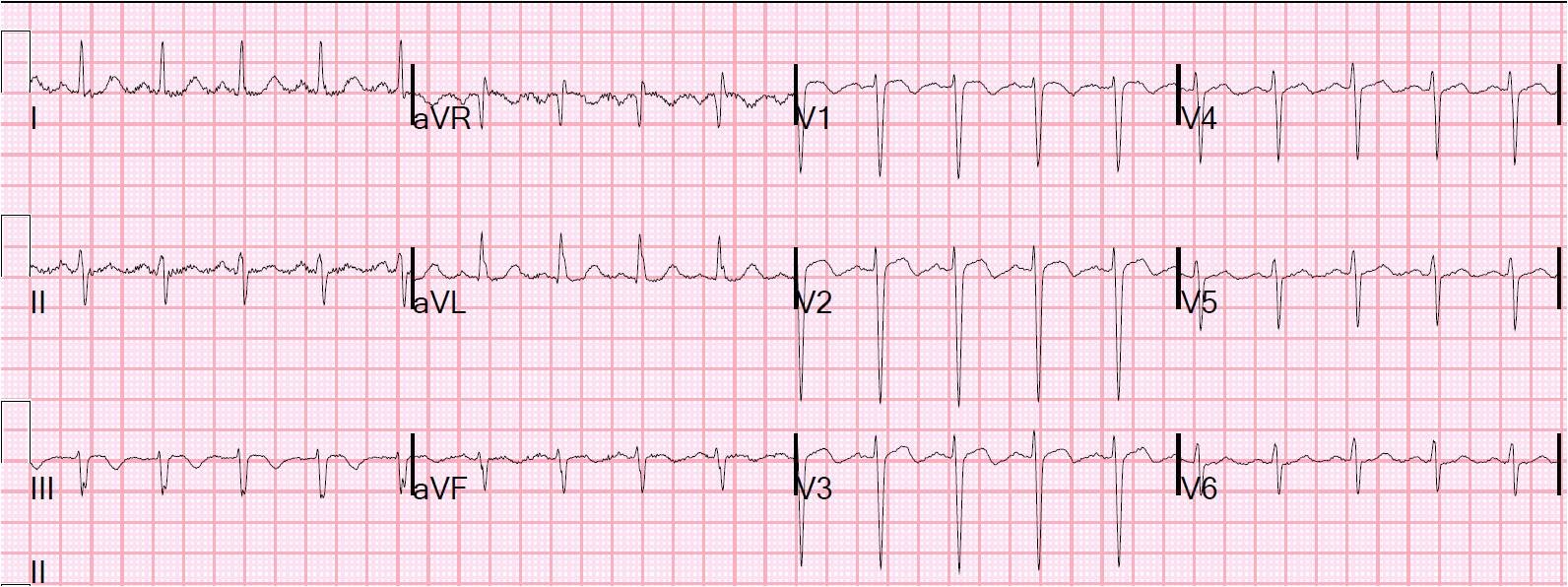
| Here, all ST segment are appropriately discordant; none excessively so. Maximum discordant ST elevation is in lead V2, (at 4 mm; but this is only 7% of a 60 mm S-wave) |
Suddenly, the patient became hypotensive. The physician (one of our fine EM residents) caring for the patient did an immediate bedside ultrasound. This showed a loculated hyperechoic pericardial fluid (blood with clot).
Patient returned immediately to cath and this confirmed a ruptured coronary artery with pericardial bleeding. A balloon pump was placed and the patient went for immediate CABG.
The circumflex was dissected and will be bypassed any moment now.