
An elderly woman with no prior known cardiac history presented with approxiately 9
hours of chest pain, much improved by arrival and essentially resolved
after a single sublingual Nitroglycerine. She was hemodynamically stable.
Here is her ECG:
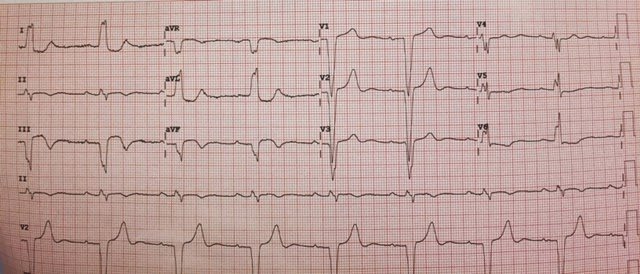 |
| There is sinus bradycardia and Left Bundle Branch Block.
The ST segments are appropriately discordant, except that in lead II there is some ST elevation; the QRS in lead II is a bit more positive than negative, so the ST segment should be negative or isoelectric, but it is elevated. This is a sign of STEMI. More importantly, though lead III has a discordant ST segment, it is out of proportion. The STE is 3 mm in the presence of a 12 mm S-wave, for a ratio of 0.25, thus highly likely to be STEMI. What is unusual is that the T-wave is concordant. This is likely due to prolonged (subacute) STEMI, or to some reperfusion (the patient is pain free after NTG), or both. There are also two signs of a fragmented QRS, which are equivalent to Q-waves in LBBB: “Cabrera’s sign” (notch greater than 50 ms on the ascending limb of the S-wave in one of V3-V5), seen here in lead V3; also “Chapman’s sign,” (notch on the ascending limb of the R-wave in I, aVL, or V6), seen here in I, aVL, and V6. |
Case continued
The physician only activated the cath lab after having a previously normal ECG faxed, and after the first troponin I returned at 41 ng/mL. This very elevated troponin shows that the infarct has been going on for quite a while and is consistent with the ECG.
He did record another ECG:
 |
| No significant change |
Outcome:
The RCA was 100% acutely occluded and was opened and stented.
Second troponin I was 70 ng/mL, Third was too high to measure.
An echocardiogram showed a new inferoposterior wall motion abnormality
Ischemic T-waves in LBBB
We showed that Concordant T-waves are weakly sensitive and specific indicators of MI [combination of STEMI and NonSTEMI] (1).
With reperfusion, even in LBBB, T-waves often invert with reperfusion. Here is a great case of STEMI in LBBB, with Reperfusion T-waves after PCI.
1. Dodd KW. Elm KD. Smith SW. Terminal T-Wave Concordance Increases the Sensitivity of Electrocardiographic Diagnosis of Acute MyocardialInfarction in Left Bundle Branch Block (full text link). (Abstract 15666) Circulation. 2014;130:A15666;
November 2014.

