I just posted this case:
Isolated “Inferior” ST Segment Depression: Not a Sign of Inferior Ischemia
Today I post another case that nicely demonstrates the significance of inferior ST depression.
A middle-aged female presented to the ED with chest pain. It had been intermittent all day.
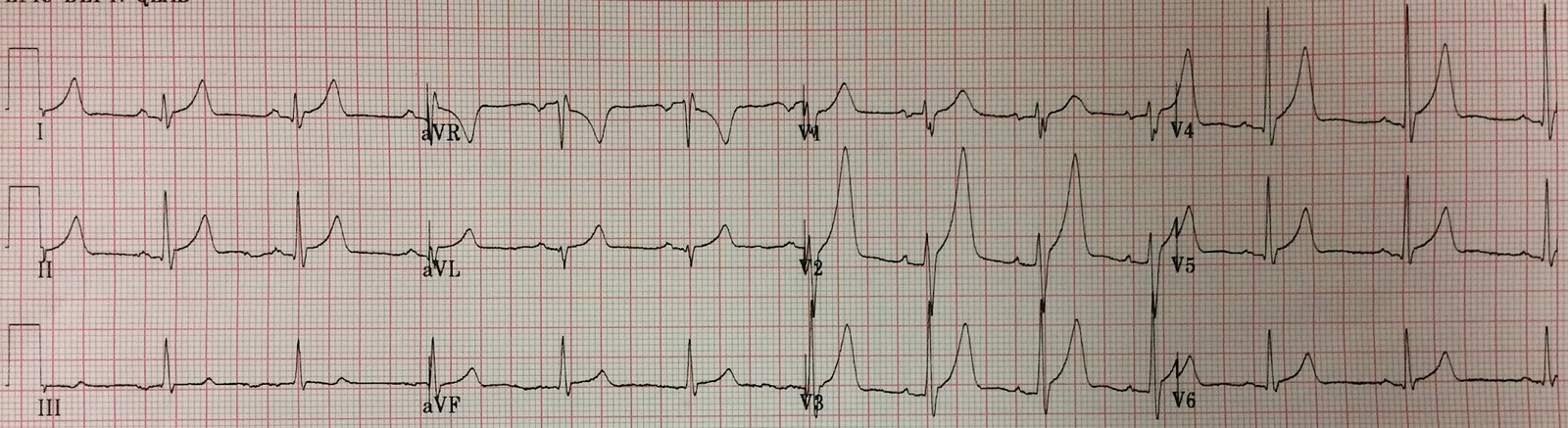
Here was her first ED ECG with active pain:
 |
| There are abnormal ST segments in “inferior” leads, and very subtle STE in aVL, with T-wave inversion. There are “down-up” T-waves in the inferior leads, which are almost always due to ischemia. |
Isolated ST depression in II, III, and aVF should be considered to be reciprocal to subtle ST elevation in aVL and to indicate that there is occlusion of the Diagonal, Obtuse Marginal, or even the LAD.
Initial troponin I was 0.65 ng/mL.
After she was initiated on ASA/Plavix/Heparin and Nitro, her chest pain resolved.
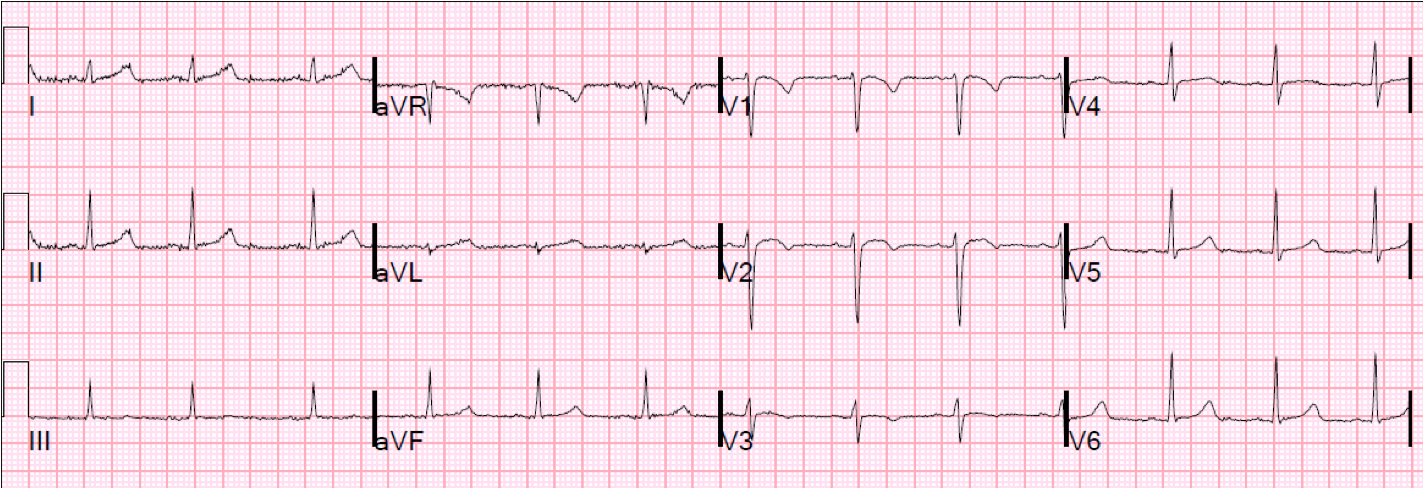
Time 40 minutes:
 |
| The ST depression is resolved. “Inferior” T-waves are now fully upright, consistent with reperfusion in the territory of aVL. Now there are Wellens’ waves in anterolateral leads, consistent with reperfusion in the proximal LAD. This strongly suggests that while the patient was having chest pain, the proximal LAD was occluded. |
She remained pain free all night.
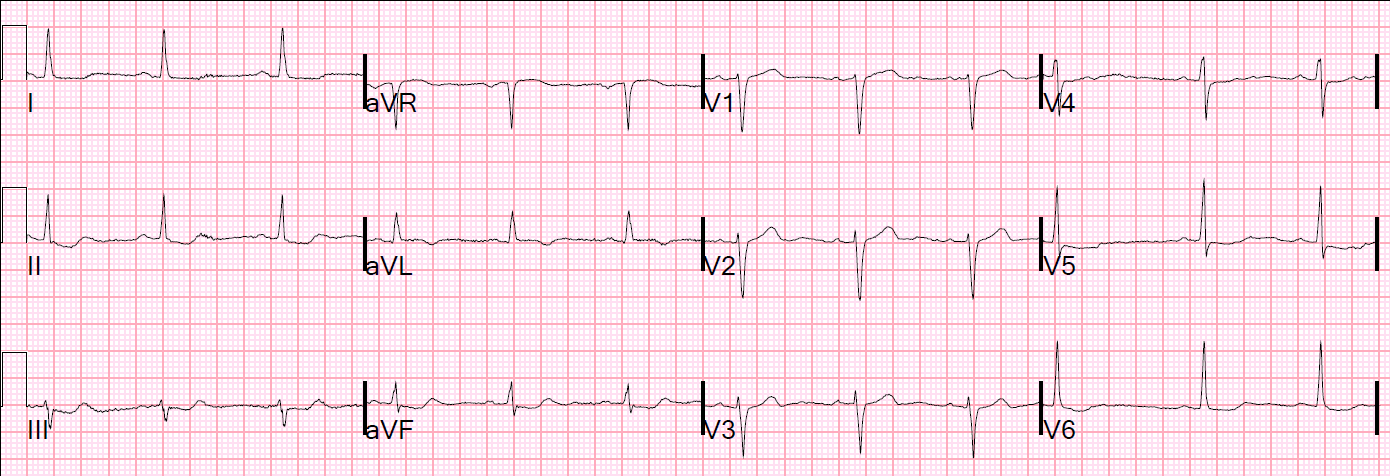
Next morning:
 |
| Evolution of T-wave inversion confirms Wellens’ waves. There is no doubt that this will be a proximal LAD lesion |
Echo showed anteroapical wall motion abnormality. Troponin I peaked at 2.5 ng/mL.
Angiogram showed 99% thrombotic stenosis with TIMI-II flow in proximal LAD. It was stented.
Comment:
At time zero, during maximal chest pain, she had a full proximal LAD occlusion. After NTG, it opened enough for adequate perfusion, chest pain relief, and T-wave inversion.
Note how subtle this occlusion was: it is only seen by some subtle ST depression in II, III, and aVF and subtle STE in aVL.
Note also that the ischemia was in the LAD territory, but the ST depression was “inferior.”