After resuscitation, he had this ECG (the rhythm is interesting, too):
 |
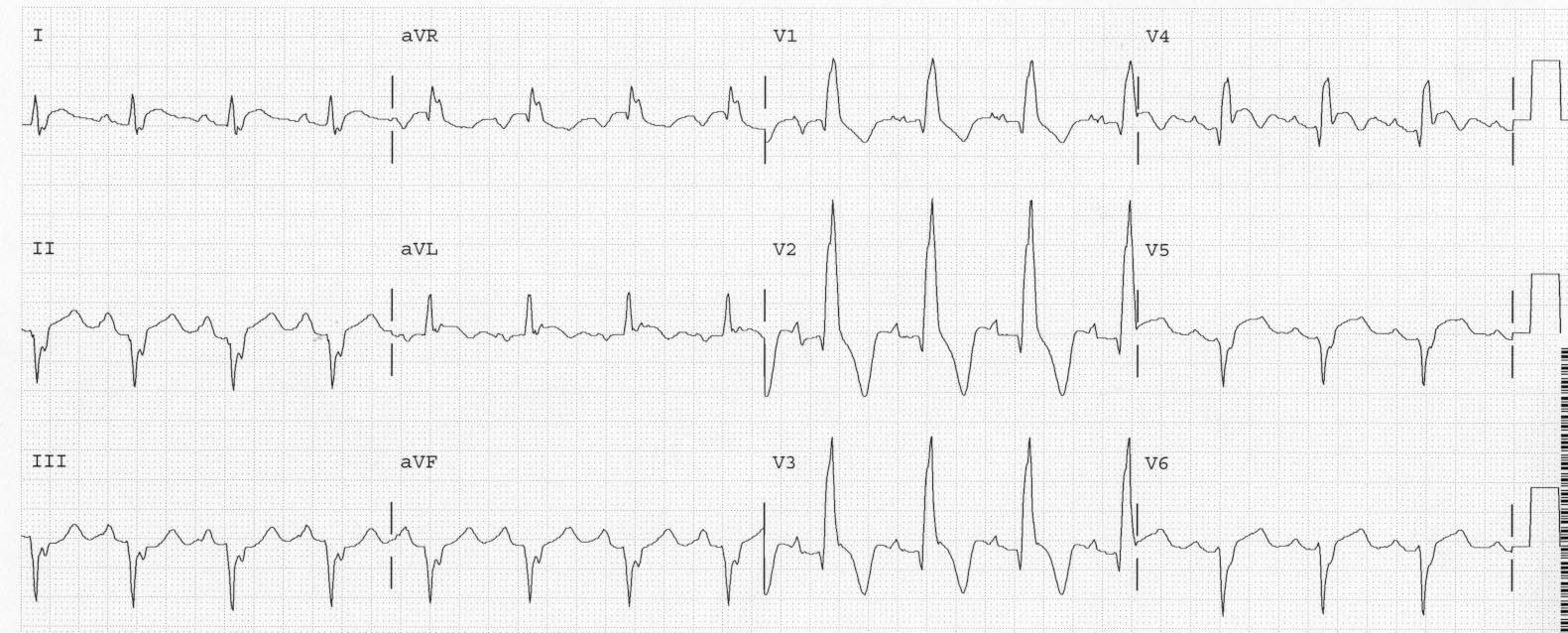
| There is sinus rhythm but the sinus rate is somewhat irregular (“sinus arrhythmia”) Whenever the sinus takes longer than about 800 ms to fire, the AV node escapes (see complexes 7, 10, and 13). Of course the most important finding is not the rhythm, but the right bundle branch block with profound ST depression most marked in leads V2 and V3, diagnostic of posterior STEMI. |
The patient was taken to the cath lab and had a distral circumflex occlusion that was opened and stented. There was a posterior wall motion abnormality.
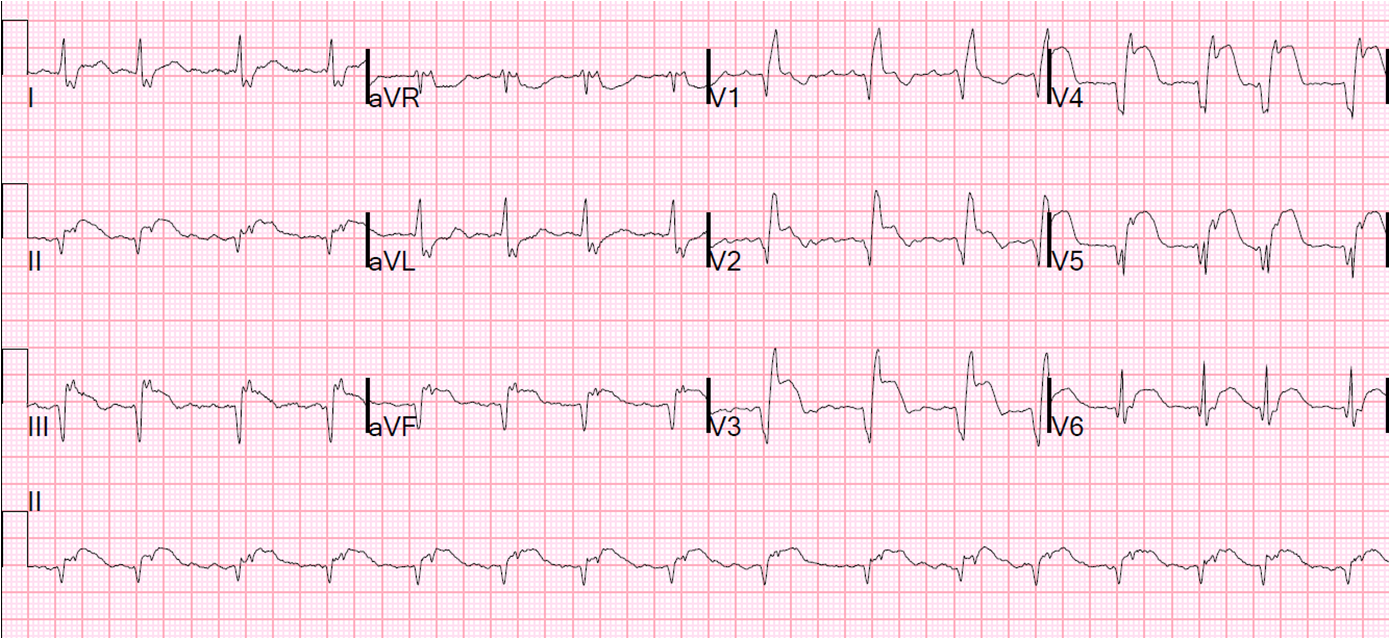
Here is a nearly identical case but with posterior leads recorded. You’ll notice in this case that the ST elevation in V9 is very subtle.
Remarks:
1. Notice the ST elevation is greatest in the right precordial leads (not left, which would more commonly signify diffuse subendocardial ischemia
2. In “isolated” posterior STEMI, there is often some subtle inferior and/or lateral ST elevation. This case is not exception: there is subtle ST elevation in aVL with reciprocal ST depression in III.
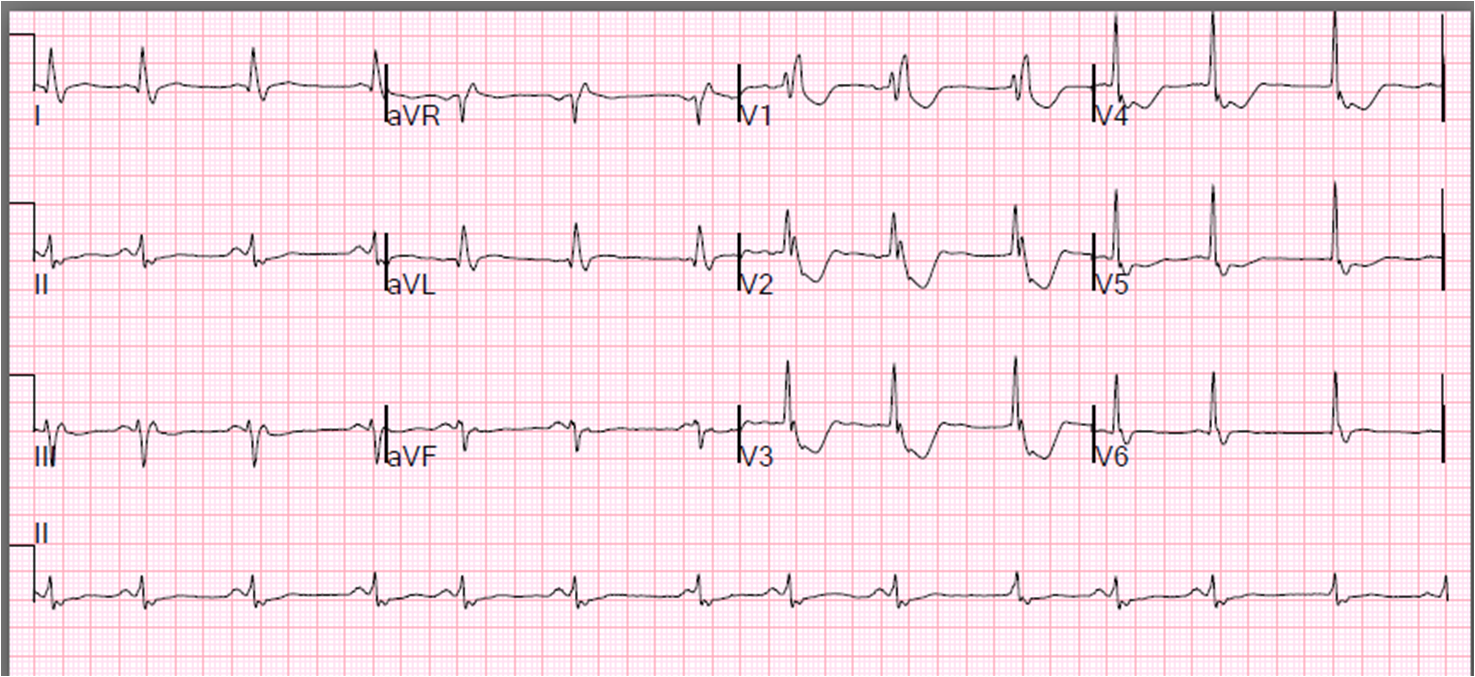
3. Although RBBB always has some ST depression in V2 and V3, in the opposite direction from the terminal R’ wave, it is usually not more than 1 mm. See the second ECG in this post for an example of the normal ST depression of RBBB.
4. The exception is with RV hypertrophy. Remember: ST segments are always proportional to the QRS, so in RV hypertrophy, the R’ wave is very large and the ST depression is proportionally large. My next post will demonstrate this.