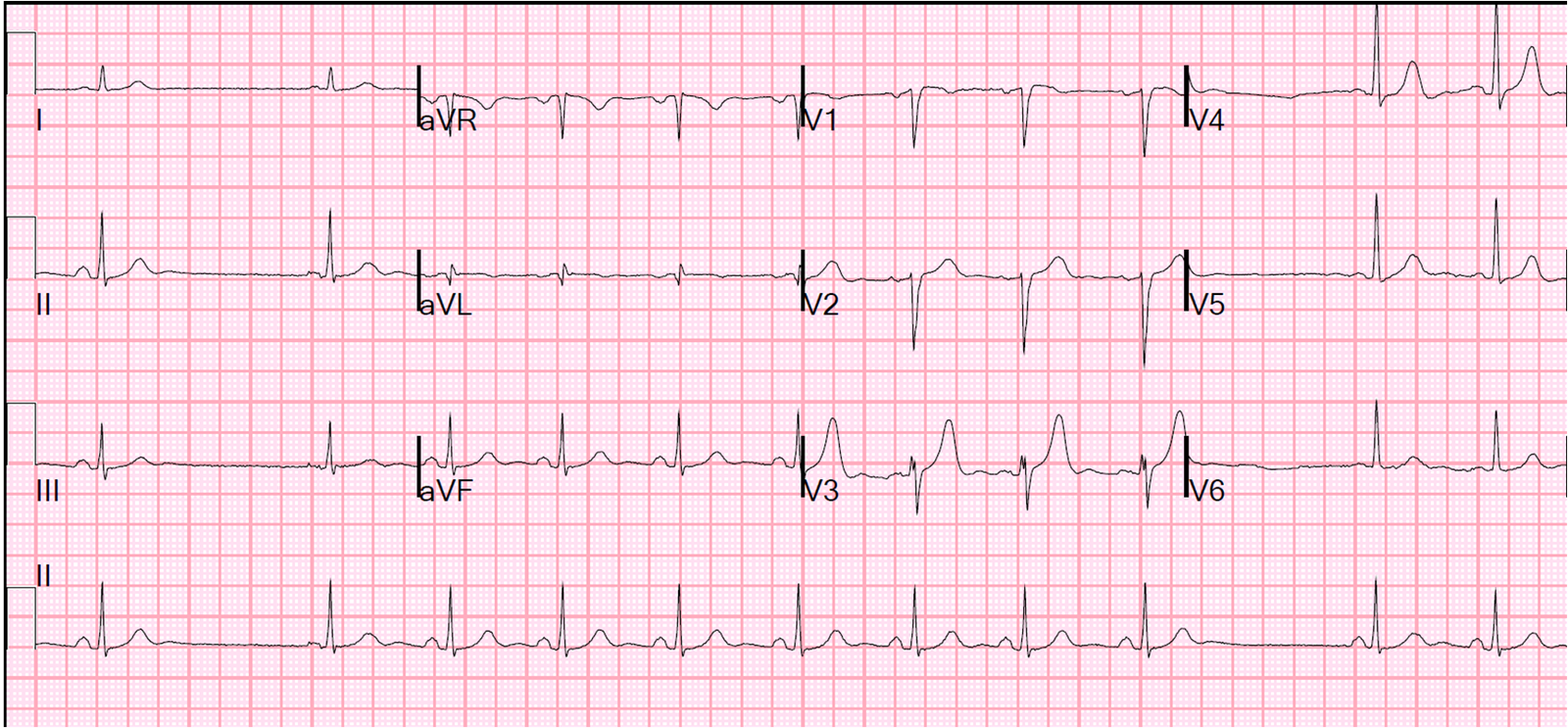
A male in his 50’s with a history of type I DM was riding his bike to work when he developed squeezing chest pressure and a sensation that “something wasn’t right.” He rode his bike directly to the ED. Here was his initial ECG:
 |
| There is very subtle, nondiagnostic (but suspicious) ST elevation in II, III, and aVF. aVL is particularly worrisome as it has a biphasic T-wave (down-up) which is almost always ischemia. Down-up is usually reciprocal to reperfusing inferior MI, though there is no evidence of reperfusion in inferior leads. V2 has a suspiciously flat/downsloping ST segment as well. |
He was given one sublingual NTG and became pain free.
There was, at this moment, no absolute indication for immediate angiography, as the patient was pain free and the ECG was not diagnostic of STEMI. However, it is nearly diagnostic of ischemia, there is minimal ST elevation, and we know that a high percentage of NonSTEMI, when they do get their angiograms at 24 hours, have an occluded infarct-related artery even though the patient has remained asymptomatic. These patients have larger infarct size, higher incidence of heart failure, lower EF, and higher mortality.
Also, it was daytime, and the cath lab was free, so why not go immediately to the cath lab?
He went for immediate cath and had a 95% thrombotically occluded mid-RCA that was opened and stented, with thrombectomy.
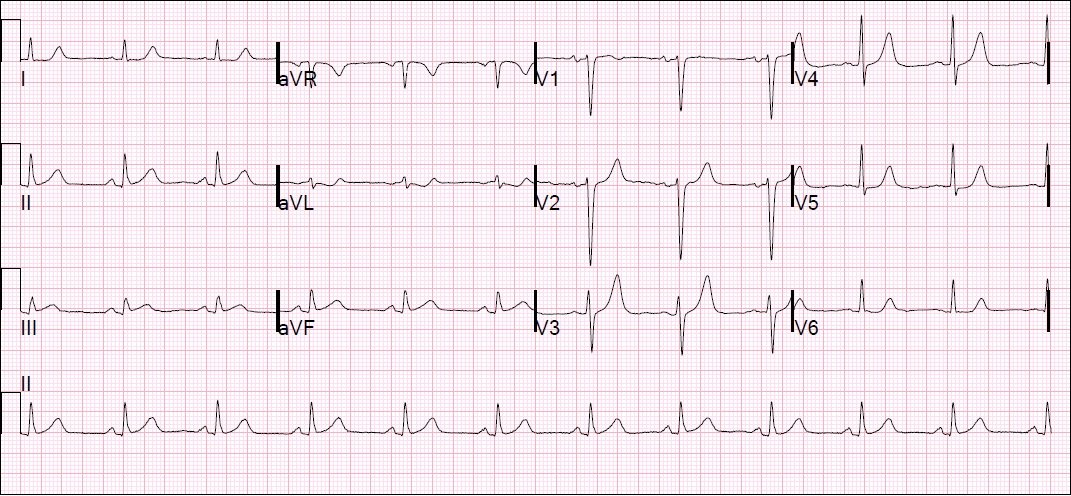
Here is the post-cath ECG:
 |
| The inferior ST elevation is entirely resolved. The T-wave in III is fully inverted (reperfusion), now with a fully upright T-wave in aVL (reciprocal to inferior reperfusion). The T-wave in V2 is now larger and more upright (reperfusion). |
The last troponin I measured was 1.0 ng/mL. The echo showed a possible mid to basal inferior wall motion abnormality. (Remember, wall motion abnormalities frequently disappear if ischemia is mild or brief)
The physician made a great call on this ECG; I like to think that, having seen so many similar cases here (as he had), made a difference.
See the very important question below in the comments section, and my answer.