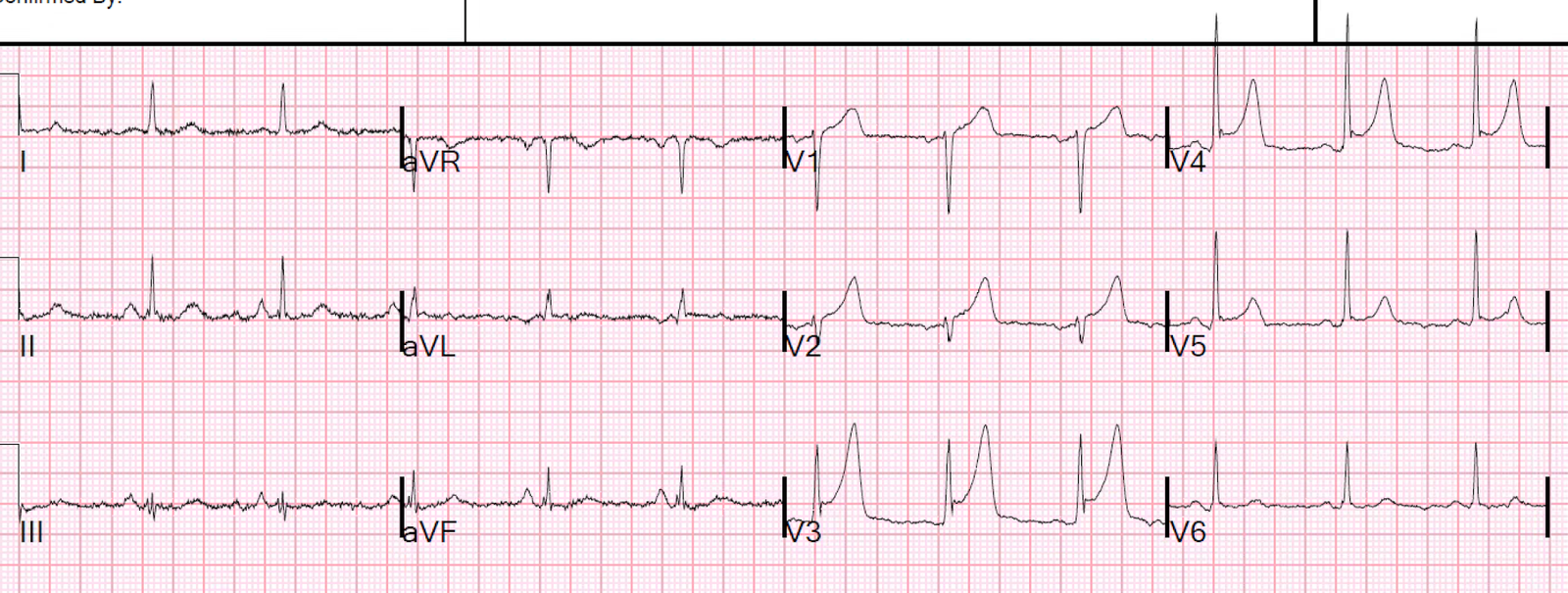
This is the ECG of a patient with a massive caffeine overdose:
 |
| What do you see? |
There is sinus tachycardia. There is some right axis deviation. There is ST depression with sagging ST segments in II, III, and aVF, and also in V5 and V6. There is what appears to be a very long QT (although the computer measured a QT of 357). This apparent long QT is a result of a large U-wave mimicking a T-wave. One should especially think of U-waves when the QT looks impossibly long. The sagging ST segments + U-wave give what I call a “wavy” appearance to the entire tracing, especially in lead II.
I am not certain of the etiology of the right axis deviation.
This tracing is a classic manifestation of hypokalemia.
See others here:
Prehospital Ventricular Fibrillation in a Young Woman. What is the Diagnosis?
And here:
https://drsmithsecgblog.com/search/label/hypokalemia
In this case, the K was 2.5 mEq/L. Caffeine causes beta agonist release and thus both beta-1 (chronotropic and inotropic) and beta-2 effects (vasodilation, bronchodilation, and hypokalemia — this is why you treat hyperkalemia with beta-2 agonists like albuterol and terbutaline).
The patient had a huge overdose, and was treated with phenylephrine (vasoconstrictor to counter the peripheral beta-2 effects of vasodilation), esmolol to counter the beta-1 activation, and benzodiazpines to counter the central CNS excitatory effects.