It is important to remember that the latest (2013) ACC/AHA STEMI guidelines removed New Left Bundle Branch Block (LBBB) as an indication for emergent reperfusion because there are too many false positives.
A reader sent this:
An elderly female presented with dyspnea, nausea, diaphoresis, and indigestion at 2am. She had a history of CAD with stents, and no history left bundle branch block.
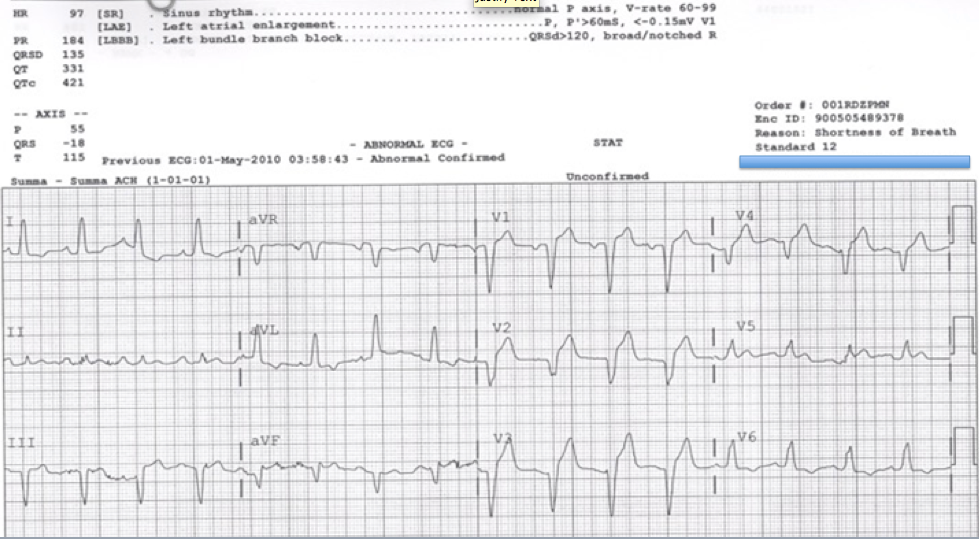 |
| There is sinus rhythm and Left Bundle Branch Block. There is not a lot of ST elevation, nowhere near 5 mm. Lead V5 possibly has some concordant STE, but there is a wandering baseline and it certainly does not come to 1 mm.
However, the ST/S ratio in V2 is high in spite of only 3 mm of STE, and it thus meets the Smith-modified Sgarbossa criteria. |
The physician wrote to me that he was suspicious of LAD occlusion, based on the modified Sgarbossa criteria, and called the interventionalist, who said, “It doesn’t meet Sgarbossa criteria.”
The emergency physician continued: “I didn’t mention your study directly but expressed my concern that this was a STEMI. We activated the cath lab. She had a totally occluded LAD with thrombus.”
See two figures below: