This 49 year old male presented with chest pain.
 |
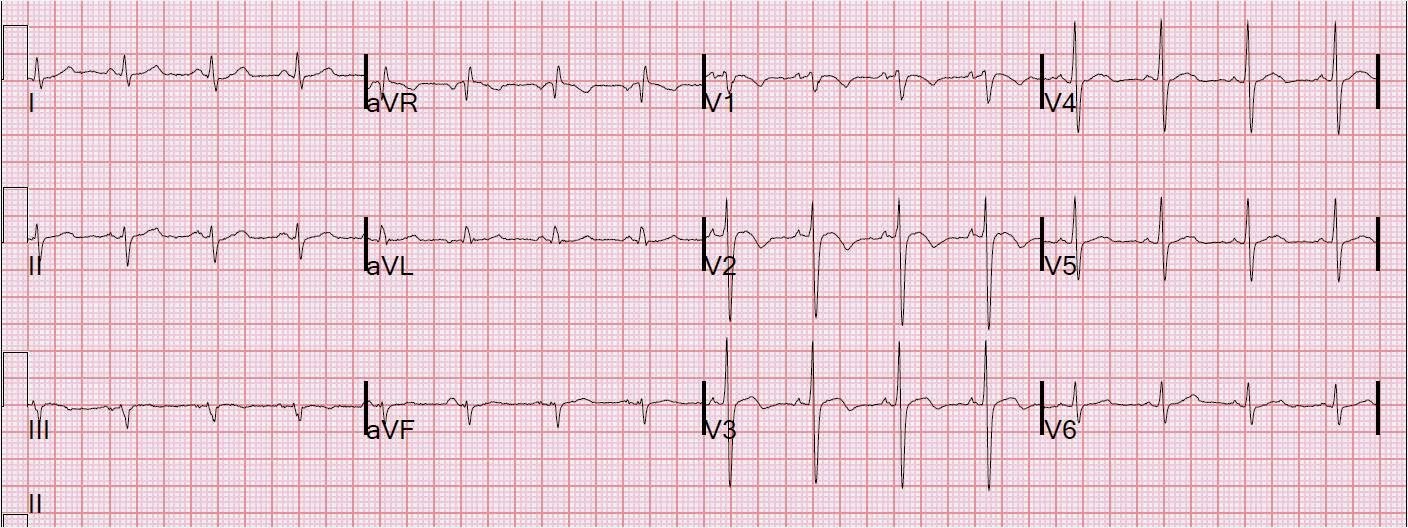
| Initial ECG: sinus with QRS of 128 ms and RBBB, though not obvious. There is T-wave inversion in lead III and a very large T-wave in aVL (very large only compared to the small size of the QRS, and it is proportional ST elevation and T-wave size that is important, not absolute size!) One would predict high lateral MI from this ECG. |
 |
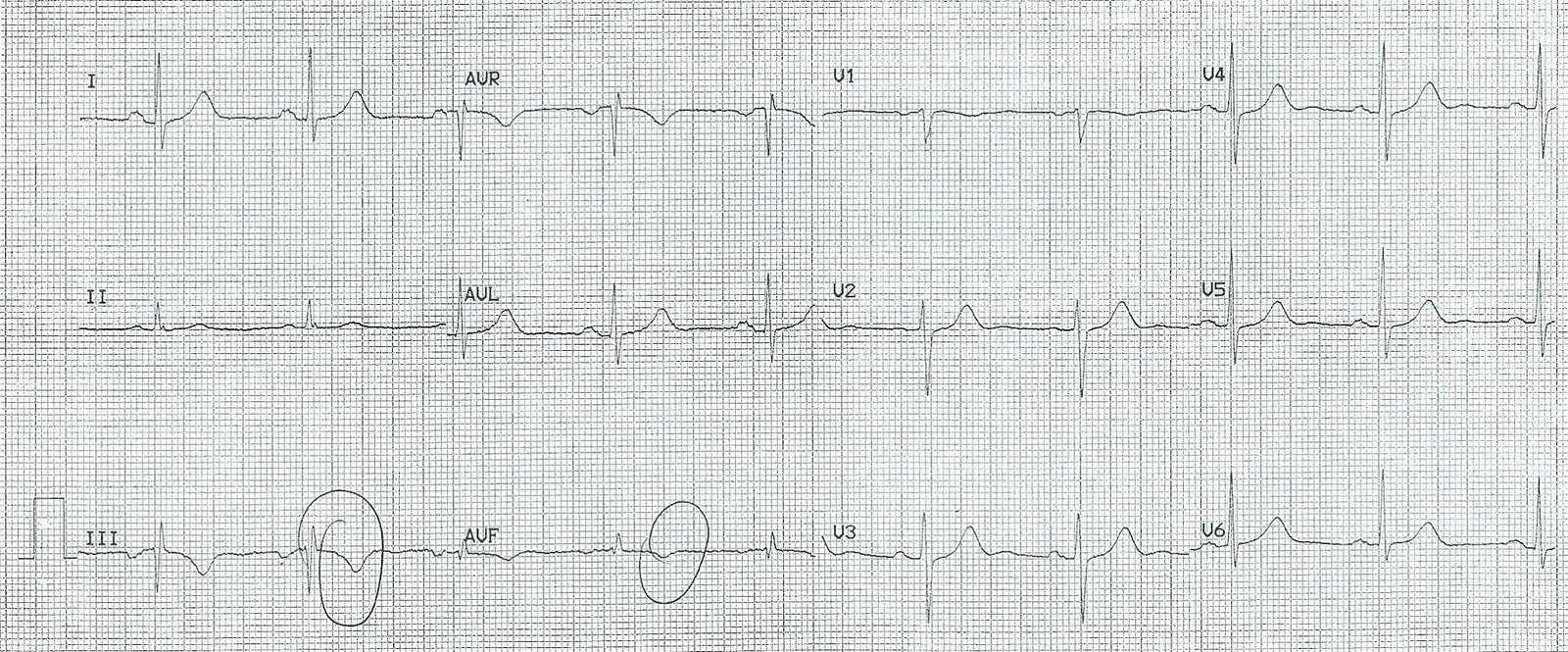
| ECG from one year ago (baseline), with QRS of 105 ms. This confirms that the RBBB and the ST-T findings in III and aVL are new. |
His chest pain resolved, then recurred, and the following ECG was recorded 70 minutes after presentation:
 |
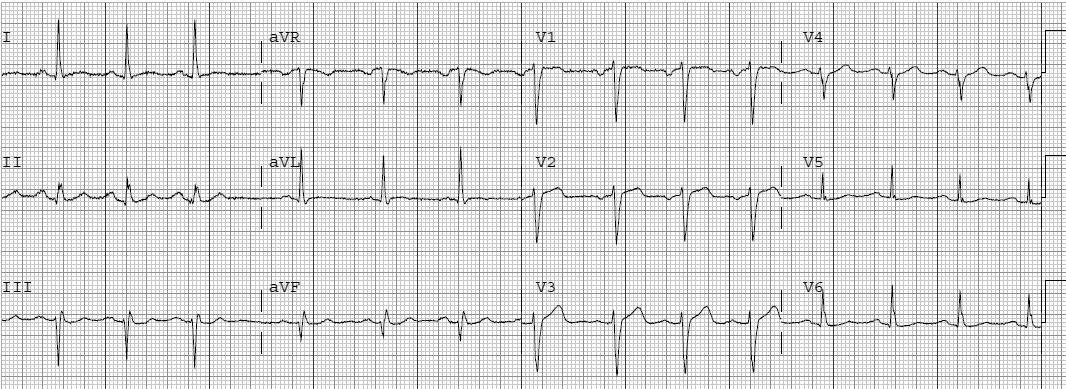
| ECG at t=70 minutes, showing dynamic T-waves (new T-wave inversion in II and deepening T inversion in III and aVF, and increasing ST depression in III, as well as increasing hyperacute T in aVL |
His chest pain resolved again, he was started on heparin, and was admitted pain free. Initial troponin I’s were 0.25 and 0.46 ng/ml.
At midnight the patient was still pain free and another ECG was recorded:
 |
| ECG at t = 8 hours, minimally changed |
At cath the next day, the culprit was a 99% proximal RCA with good flow. There was a posterolateral (RPL-1) branch off of this RCA with a 90% stenosis.
I have changed the outcome of this case because there is uncertainty as to whether, angiographically, there was ischemia to the inferior (RCA) or the lateral wall (RPL-1). My assessment from the ECG is that it was high lateral, with reciprocal inferior ST findings. But the angiographer thinks that it was the inferior wall that was most ischemic.