This patient presented with severe DKA.
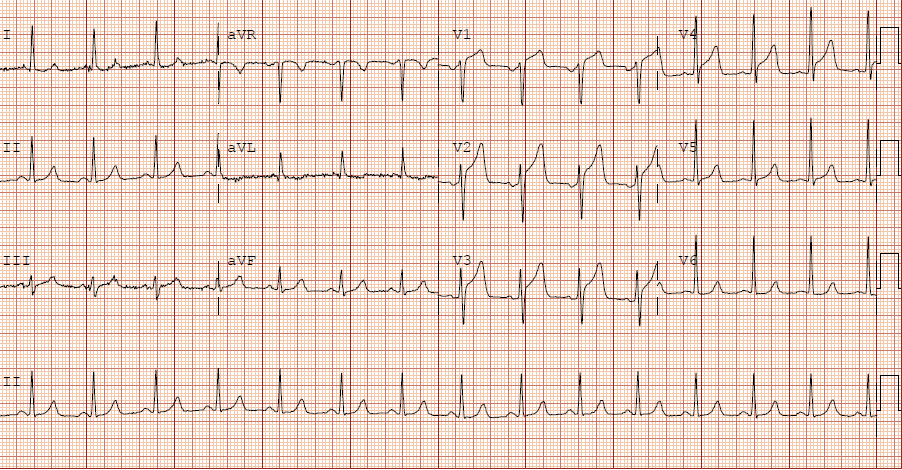
Here is the ECG:
 |
| Sinus tachycardia.
What do you think? |
The computer and physician reader wrote: “ST depression, consider subendocardial injury.”
The computer read the QT as 365 ms and the QTc as 424 ms. What else?
I read the QT interval as somewhere between 480 and 580 ms, depending on the complex, with a QTc (Bazett correction) of 630 – 763 ms. There is a very prominent U-wave and some of what may appear to be a QT interval is a QU interval. So the real QT is shorter, but the computer does not mention the U-wave, and the U-wave is as important as the T-wave in predicting cardiac dysrhythmias.
This is an extremely dangerous ECG.
The K returned at 1.9 mEq/L.
This is extremely low for DKA.
K in DKA is usually high from shifting out of cells, and will go lower as it shifts into cells during treatment.
Therefore, hypokalemia in the setting of DKA is truly life threatening and must be treated aggressively.
When the ECG shows the effects of hypokalemia, it is particularly dangerous. In spite of aggressive K replacement, the patient went into ventricular fibrillation.
Discussion
See this post: STEMI with Life-Threatening Hypokalemia and Incessant Torsades de Pointes
I could find very little literature on the treatment of severe
life-threatening hypokalemia. There is particularly little on how to
treat when the K is less than 2.0, and/or in the presence of acute MI.
Here are the American Heart Association Guidelines:
Part 10.1: Life-Threatening Electrolyte Abnormalities
“The treatment of hypokalemia consists of minimizing further potassium
loss and providing potassium replacement. IV administration of
potassium is indicated when arrhythmias are present or hypokalemia is
severe (potassium level of less than 2.5 mEq/L). Gradual correction of
hypokalemia is preferable to rapid correction unless the patient is
clinically unstable.
“Administration of potassium may be empirical in emergent conditions.
When indicated, the maximum amount of IV potassium replacement should be 10 to 20 mEq/h with continuous ECG monitoring during infusion A more concentrated solution of potassium may be infused if a central line is used, but the tip of the catheter used for the infusion should not extend into the right atrium.
“If cardiac arrest from hypokalemia is imminent (i.e., malignant
ventricular arrhythmias are present), rapid replacement of potassium is
required. Give an initial infusion of 10 mEq IV over 5 minutes; repeat
once if needed. Document in the patient’s chart that rapid infusion is
intentional in response to life-threatening hypokalemia.”
CASE: Prehospital Cardiac Arrest due to Hypokalemia
I recently had a case of prehospital cardiac arrest that turned out to be due to hypokalemia.
We could not resuscitate her, but we did have excellent perfusion with LUCAS CPR, such that pulse oximetry had excellent waveform and 100% saturations, end tidal CO2 was 35, and cerebral perfusion monitoring was near normal throughout the attempted resuscitation.
During the resuscitation, I ordered 10 mEq KCl push, but the patient received 40 mEq of KCl, push (far more than recommended) The resident had ordered 40 mEq and that is what the nurses heard.
Is 40 mEq too much? Or the right amount?
Contrary to my expectations, after pushing 40 mEq, the K only went up to 4.2 mEq/L.
What is the right amount of K to push in life-threatening hypoK?
In a 70 kg person, there are 5 liters of blood and 3 liters of serum. Since it takes some time (how long?) for K to shift out of the intravascular space into the interstitial space and then into the intracellular space, 3.0 mEq of K pushed fast and circulated theoretically would raise serum K immediately by 1.0 mEq/L, and 10 mEq would increase it by 3.3 mEq/L, from 1.9 to 5.2. Thus, 40 mEq should raise it by 13 mEq/L!!
But this is before redistribution to the interstitial space.
As I indicated above, in our cardiac arrest case, after pushing 40 mEq, the K only went up to 4.2 mEq/L.
There are about 13 liters of extracellular fluid in a 70 kg person (10 liters interstitial fluid + 3 liters serum). So if K redistributes very quickly to this extracellular space, then 40 mEq is appropriate.
The difficulty is in estimating the ongoing shift. As you infuse K, it will start to shift into depleted cells and the serum K will fall again rapidly. Thus, it is critical in patients like this to repeatedly and rapidly, after each bolus, measure the K, and supplement as needed.
Total Body Potassium: a 70 kg person has about 7500 mEq of total body K, but the extracellular fluid has only about 45 mEq! Of course the difficulty with K
replenishment is that the total body stores may be depleted by far more
than can possibly be quickly repleted. The estimated deficit associated
with a serum decrease from 4.0 mEq/L to 3.0 mEq/L is 100-200 mEq of total
body K, and from 3.0 mEq/L to 2.0 mEq/L, the associated loss is double, at 200-400
mEq.* [Sterns RH, et al. Internal potassium balance and
the control of the plasma potassium concentration. Medicine (Baltimore)
1981;60:339-54].
But 100 mEq given all at once by bolus, could (before any redistribution to interstitial space) raise the serum K by 33 mEq/L (and be immediately fatal)!!
*The NEJM review referenced below (and ACLS, for what that is worth), states that, on average, in a “typical” 70 kg person,
the serum K falls by 0.3 mEq/L for every 100 mEq total body deficit.
However, this review references the Sterns article above, which by my
reading does not state this.
Further complicating the issue is that severe hypokalemia can result in
rhabdomyolysis and subsequent K release, with resulting hyperkalemia!
Here is review of hypokalemia from the NEJM,
but it is mostly about etiology, and says little about rapid
replacement in life-threatening hypokalemia EXCEPT to emphasize how
dangerous rapid replacement is.