For more on hyperkalemia, click here (includes a great case of incessant ventricular tachycardia).
For more on early repolarization, see these cases:
For differentiation of early repol from LAD occlusion, click here.
Hyperkalemia resulting in cardiac arrest
Although there is little high quality data on differentiating these entities, some general insights are useful, and illustrated with the following cases:
Case 1
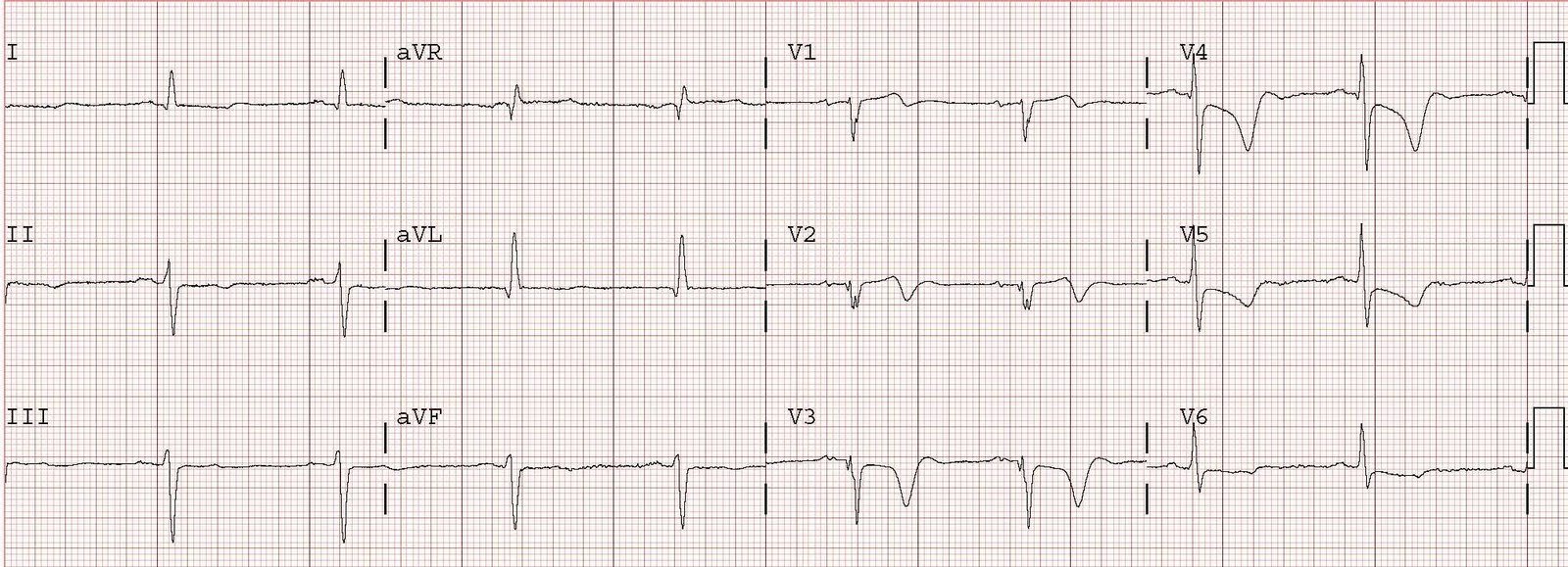
The first ECG is one of a 27 y.o. patient who presented with ventricular fibrillation.
ECG #1, hyperkalemia
Because of the large T-waves, this ECG was interpreted as “hyperacute T-waves”. However, these T waves are pathognomonic of hyperkalemia because they are peaked, “tented”, come to point, have a very flat ST segment, and there is a long QRS (114 ms).
Conventional wisdom (with no hard data, to my knowledge) says that when hyperkalemia has a normal QRS that the QTc should be short. This idea conforms with the complex electrophysiology of hyperkalemia, but may not always be true in real life.
Case 2
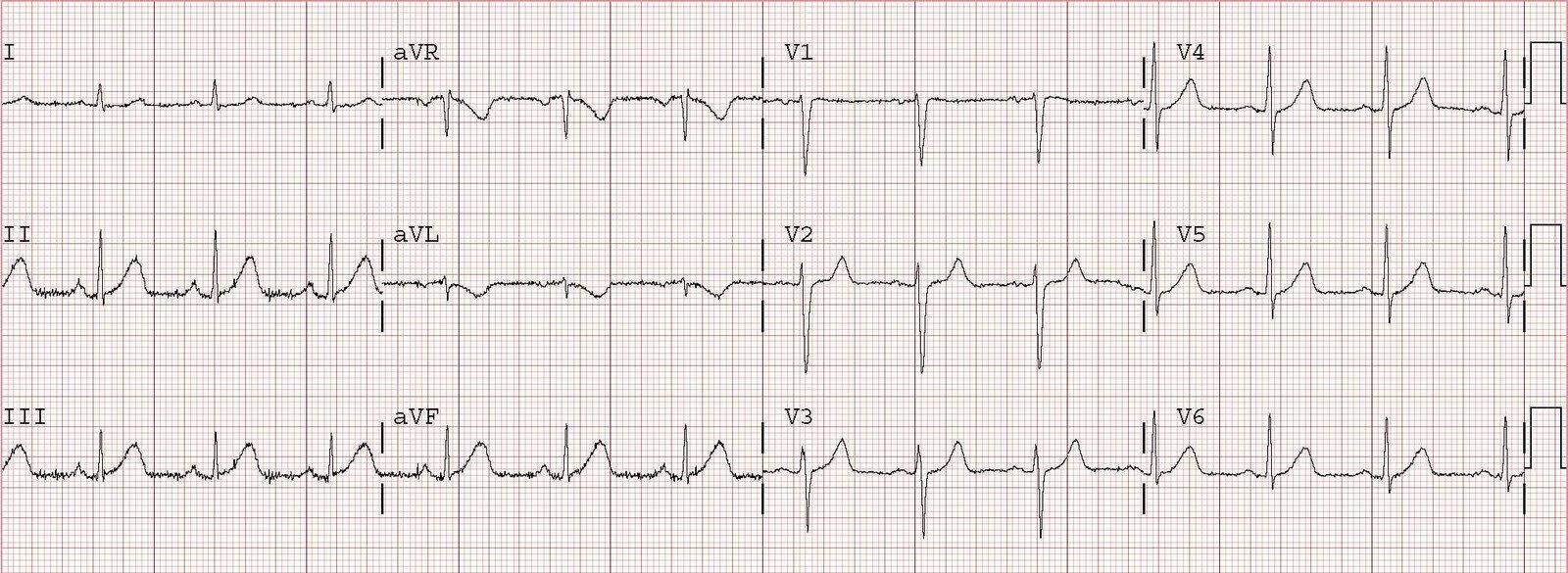
ECG #2, LAD occlusion

In this ECG#2 above, the T-waves are slightly more blunt at the peak, there is a normal QRS duration with a long QTc at 450 ms, the ST segment is straightened (less upward concavity, steeper ST segment) which results in an area under the curve (integral) that is larger than in either hyperkalemia or early repol (i.e., the T-wave is “fat”)
Case 3
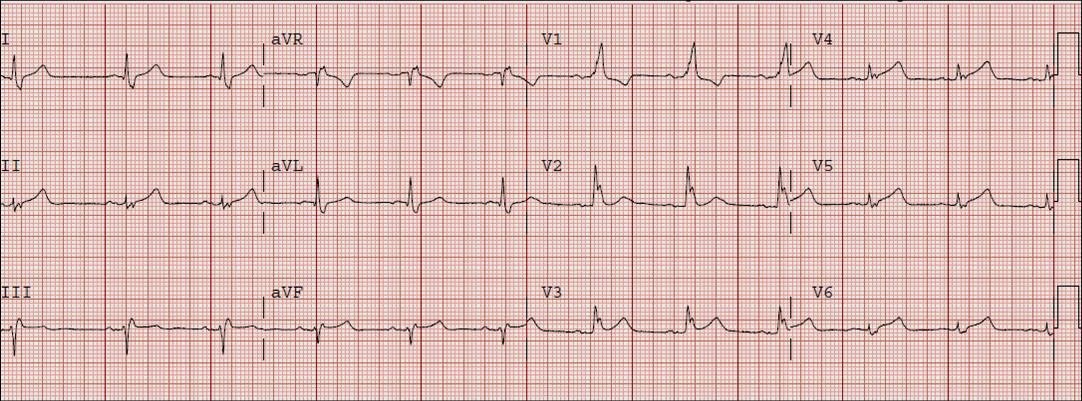
This patient presented feeling moderately ill:
EKG #3, hyperkalemia, QTc 497 ms, QRS 102 ms (normal is less than 110ms)
 |
| See V4 especially. The ST segment is horizontal until it abruptly rises to a very peaked T-wave. The T-wave is “tented” to a point. |
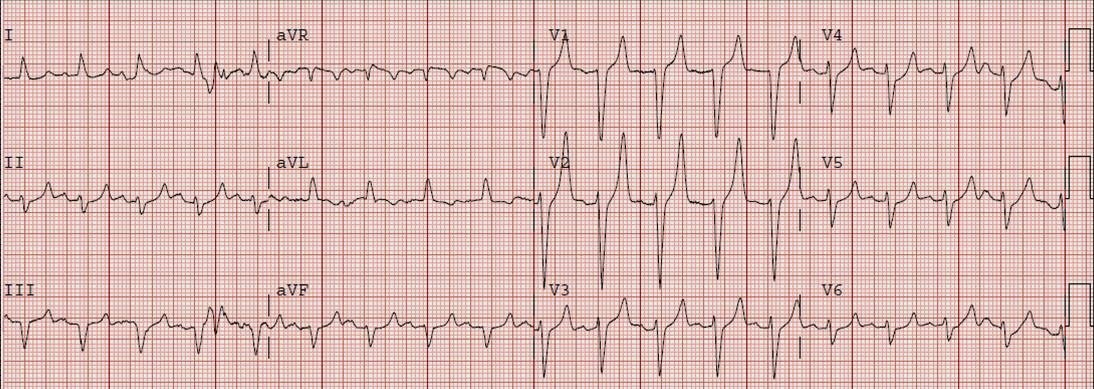
Due to the peaked T-waves, the residents were immediately concerned for hyperkalemia and sought an old ECG, which they immediately found (shown below, ECG #4):
EKG #4, early repolarization, QTc 455 ms, QRS 82 ms
 |
| Notice the ST segments here are not nearly as flat, and the rise to a peaked T-wave, especially in lead V4, not nearly as steep |
After viewing this previous ECG, and knowing that the K was 4.5 at the time it was recorded, the residents believed that the peaked T waves in ECG #3 were this patient’s baseline. It is true that early repolarization has tall and relatively peaked T waves, but not to the extent seen in ECG #3. Without seeing them side by side, it is hard to appreciate the difference, but the ST segment in V4 in EKG #3 is flat, making the base of the T wave much more narrow.
This patient, then did not get immediate treatment for hyperK.
I saw these ECGs at a slightly later time than the resident, recognized the difference and, worried about the patient, started toward his bedside. As I was approaching the patient, he had a v fib arrest. He was immediately resuscitated, then his K returned at 7.0 mEq/L. This was a presumed hyperkalemic arrest.
Some say you don’t need to treat hyperK unless there is QRS widening. They claim that peaked T-waves are not enough. This is only one case, and anecdotal, but we found no other etiology of arrest in this patient. I always treat immediately if the ECG is affected by hyperK.
In addition, the QRS duration difference is important; the difference in QTc seems to defy conventional wisdom.
There is a definite difference, with EKG#3 pathognomonic for hyperkalemia.