A young otherwise healthy man presented with 4 hours of sharp 10/10 substernal chest pain. It has been constant since then. He looked ill and diaphoretic. BP was 160.
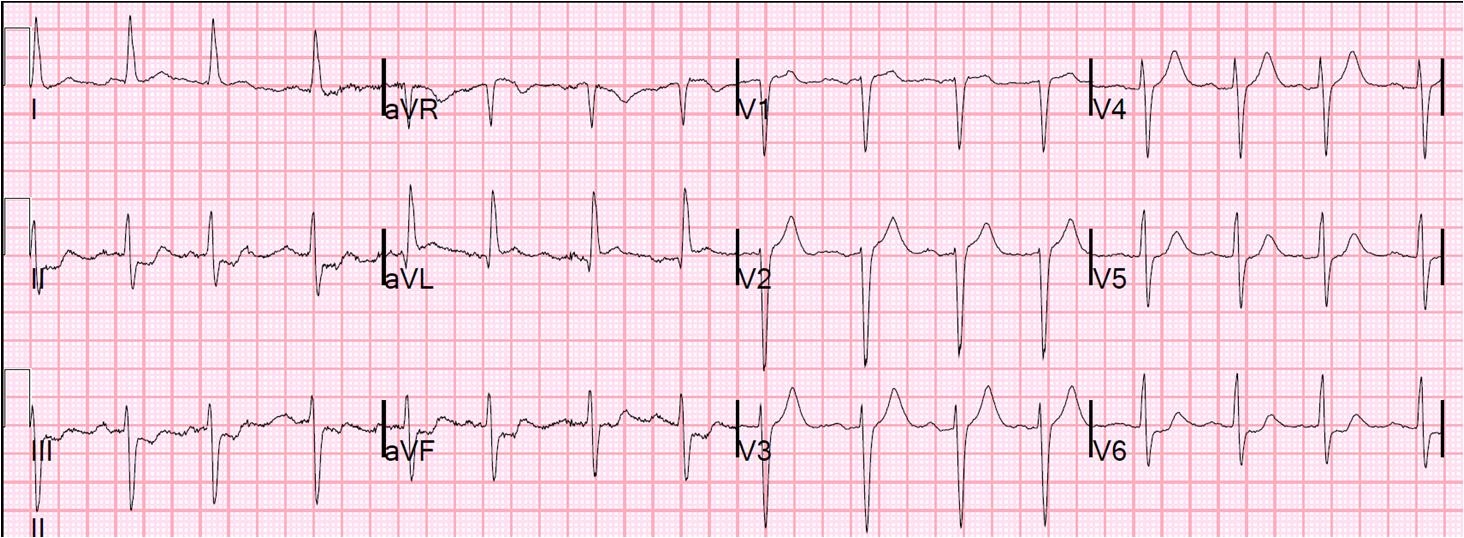
Here is his ECG at t = 0:
 |
|
|
This ECG is diagnostic of anterior STEMI. And the Cath lab was activated immediately.
But there was some doubt as to whether it might be pericarditis because
of the ST elevation in I and II, without ST depression in III. Add
that to “sharp” pain and a 33 year old, and it is easy to convince
yourself that this is, indeed, pericarditis.
However, look closely!
1. There is a fragmented QRS in lead V2 (potential goes up, then down, then up again). This is a good sign for myocardial infarction and does not happen in pericarditis.
2. The voltage in V2 is very small. This is a sign of MI, either acute or old.
3. There is terminal QRS distortion in V2 and V3 (you might dispute that V3 has what looks like a J-wave, but I would argue this is not what a true J-wave looks like)
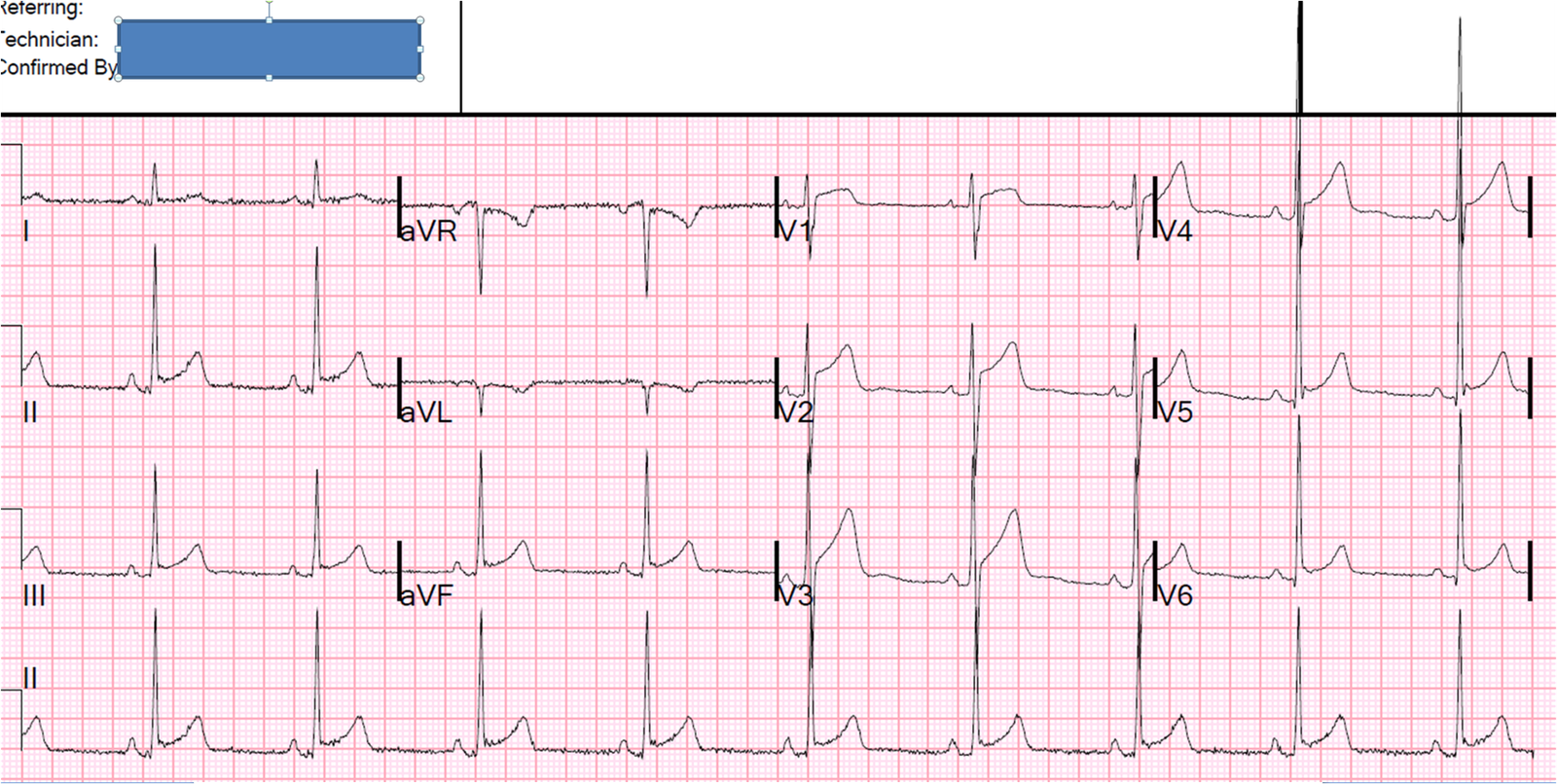
After nitroglycerine, his systolic BP was 120 and his pain was improving. Heparin and aspirin were given. Another ECG was recorded at t = 27 minutes:
 |
|
|
The patient went to the cath lab and had an 80% occluded mid LAD with fresh thrombus. It was a “type III” LAD, meaning it wraps around to the inferior wall. The distal inferior apical LAD was cut off by distal embolization from LAD culprit. The Right Posterior Descending Artery off the RCA was small, so that the RCA did not adequately supply the inferior wall.
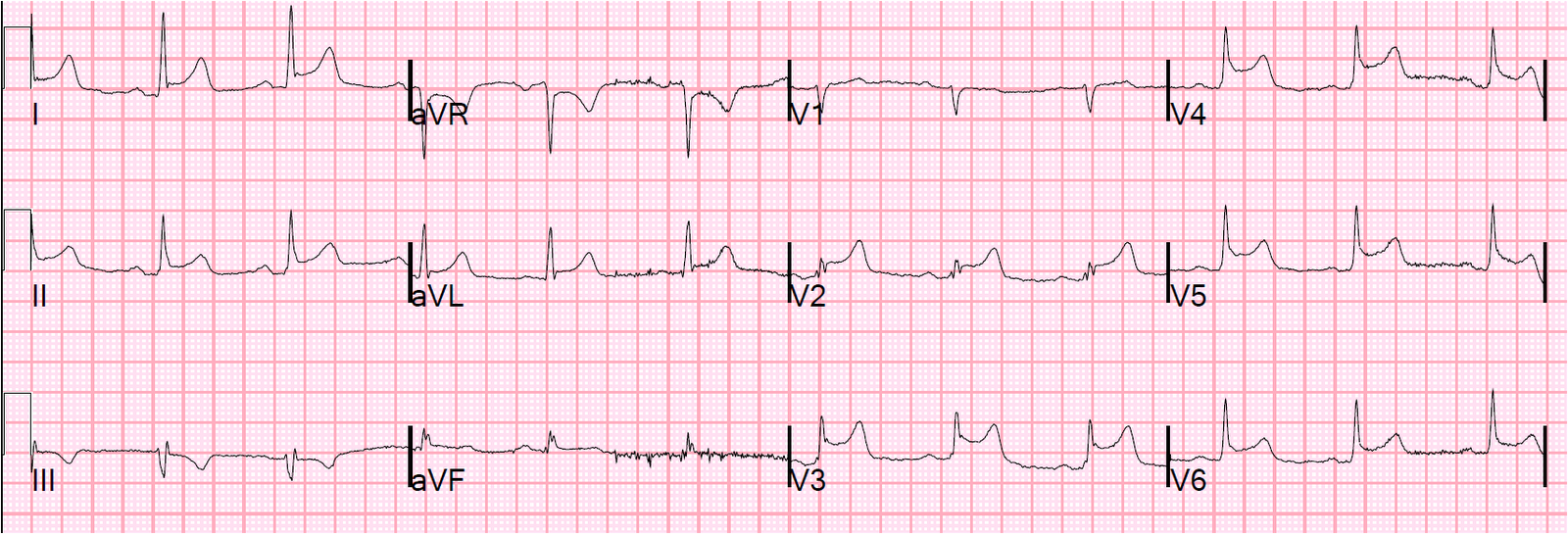
Thanks to spontaneous reperfusion (helped by aspirin and nitroglycerin), the artery was open and the peak Troponin I only 12.2ng/mL.
Echo showed an apical, but not inferior, wall motion abnormality. This is likely because 1) the ischemia to the inferior wall was only partial and 2) it reperfused quickly.
Lessons:
1. Occlusion of a Type III (wraparound) LAD that supplies both the anterior and inferior wall can have “widespread ST elevation” that can be confused with pericarditis.
2. The QRS is at least as important as the ST segment in diagnosing STEMI