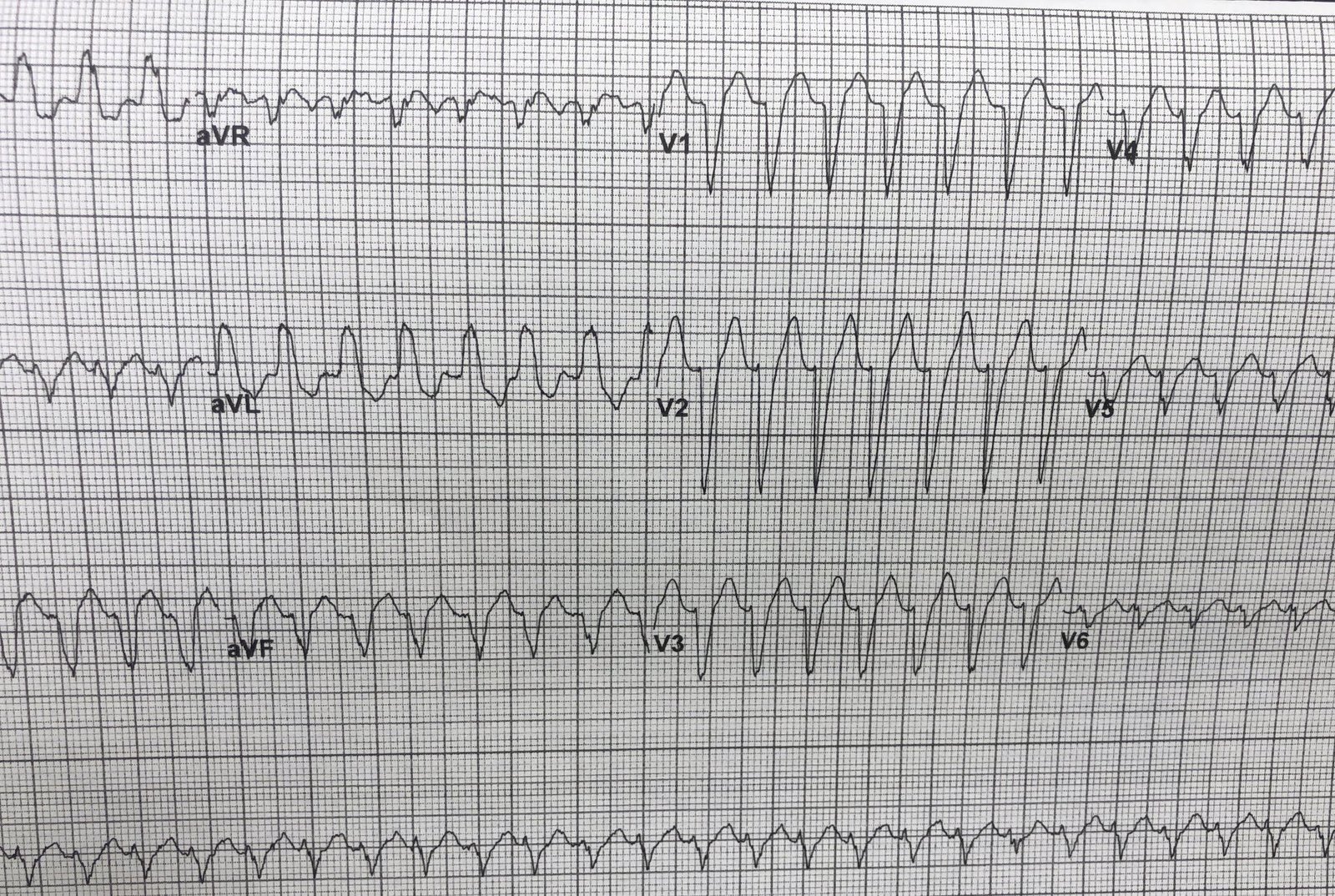
An elderly patient had a pre-procedure ECG (ECG-1). She was asymptomatic. The patient had known Left Bundle Branch Block (LBBB) and atrial fibrillation (see ECG-2 below), and was rate controlled on metoprolol.
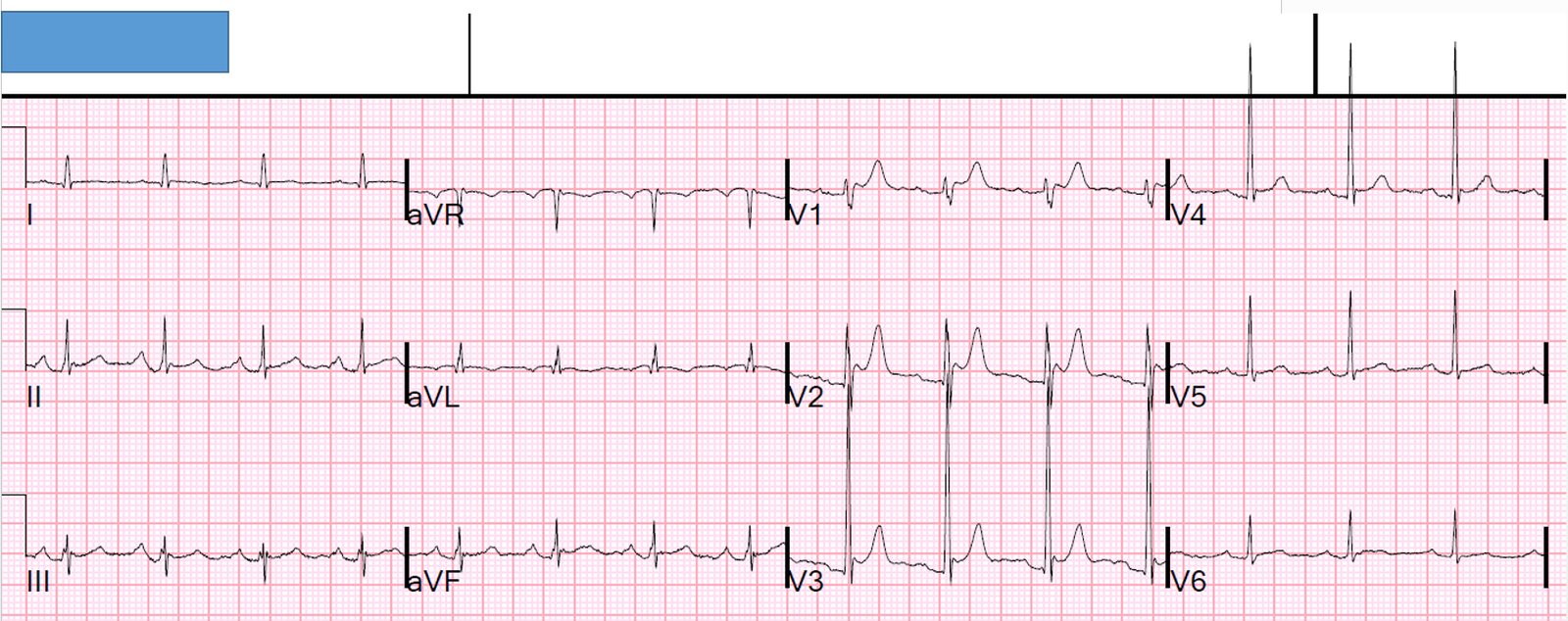
ECG-1
 |
| What is the problem? |
ECG-2 (previous for comparison):

There are enormous U-waves, best seen in V1-V3, but also in V4 and V5. This was seen by the overreading cardiologist. The cardiologist called the The K was checked and it was 1.9 mEq/L.
The patient was sent to the ED for hypokalemia.
While being assessed and having potassium orally and IV, her heart rate dropped to 30 beats per minute (2 second pauses). She was dizzy whenever not supine (symptomatic).
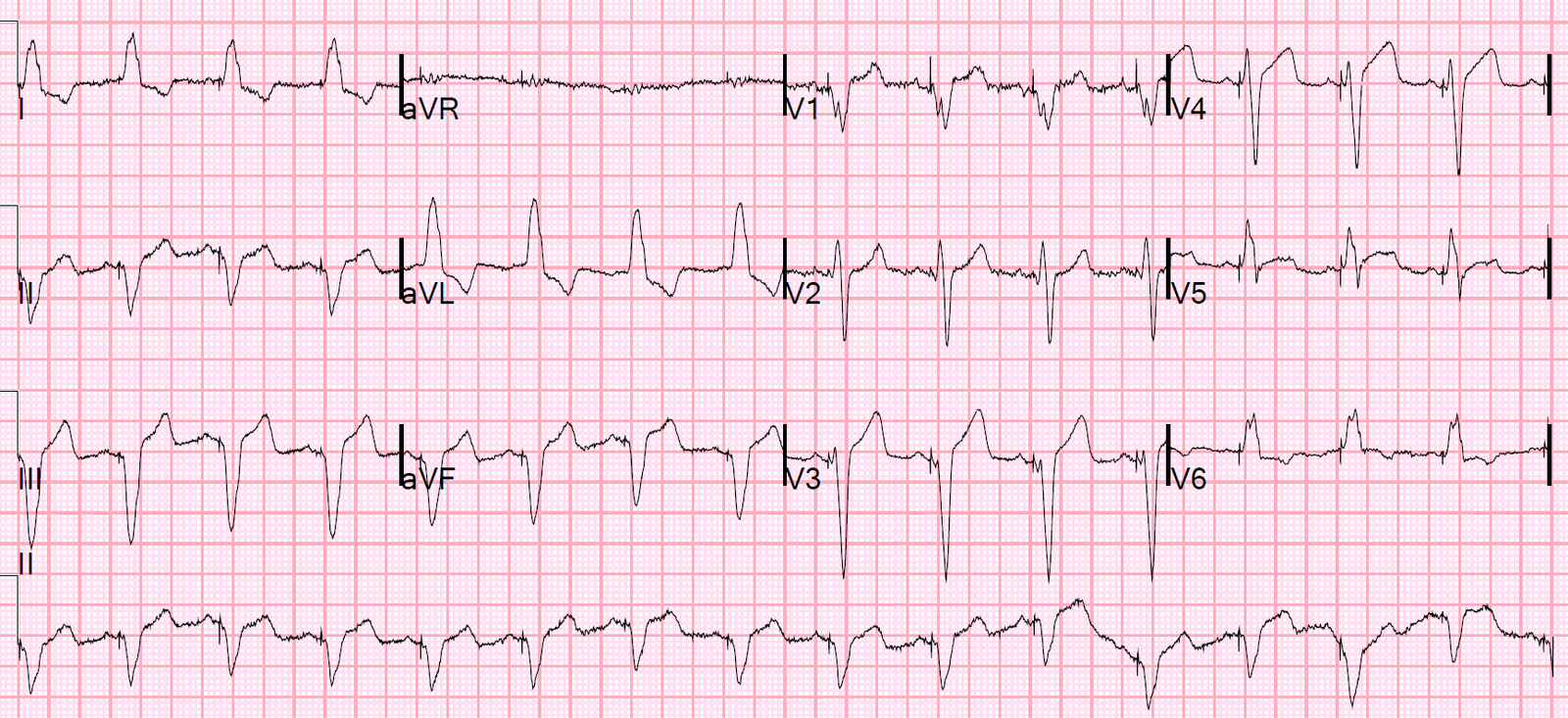
This 12-lead ECG (ECG-3) captures her at a heart rate in the 40s, but the monitor at times had a much slower rate.
ECG-3:
 |
| Still in atrial fibrilation with a slow ventricular response and LBBB, and with large U-waves. This implies the AV node is not working well. |
What do you want to do?
This is what we did:
We gave atropine and the heart rate responded perfectly, with rate rising to 70-80.
After replenishment of KCl, orally and IV, the heart rate stabilized and the etiologies of the hypokalemia were also corrected.
The patient was discharged the next day.
Severe hypokalemia causes life threatening dysrhythmias. At exactly what level one is at risk of such dysrhythmia is uncertain, but certainly any K below 2.0 is life threatening. Probably under 2.5 is life threatening. I believe that any hypokalemia that results in ECG abnormalities such as large U-waves, long QT, or ST-T abnormalities is potentially life threatening.
There are few reports of AV block due to hypokalemia, but it has been described. It is also rare to see U-waves in the setting of LBBB.
Two case reports of hypokalemia associated with AV block