Question:
This tracing shows (choose one from the list below)
a) atrial bigeminy with aberrant conduction
b) ventricular bigeminy
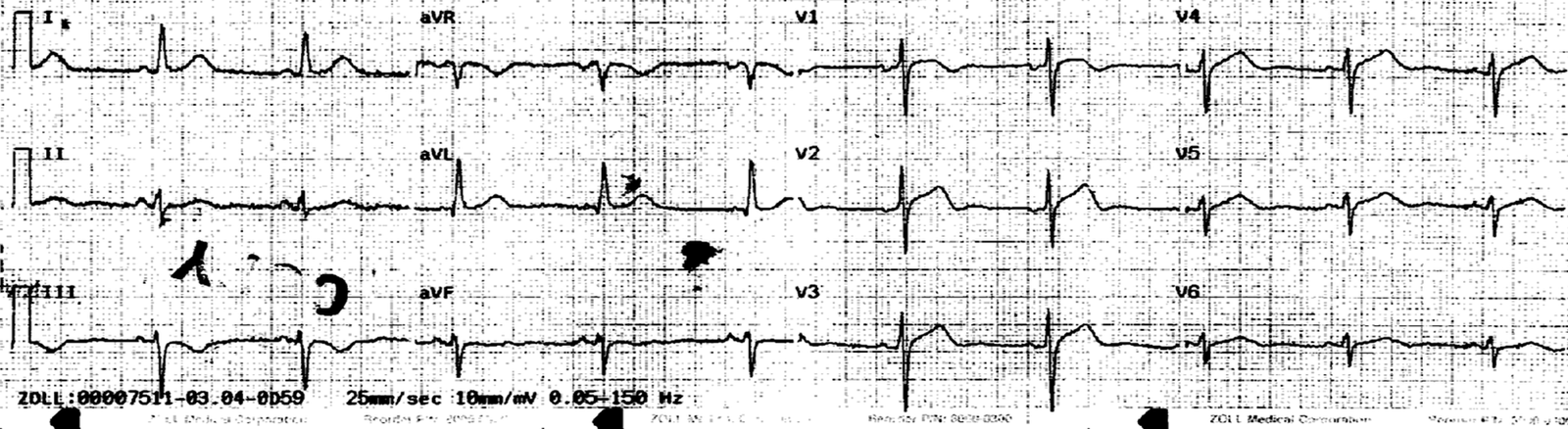
Annotated ECG:
 |
| Answer: a) atrial bigeminy with aberrant conduction. |
Discussion:
Every other QRS is wide, different looking from the sinus beats and, at a quick
glance, the tracing seems to show ventricular bigeminy. However, careful
observation reveals a prematurely occuring P wave (↓) in front of these wide QRSs and this
is an examle of atrial bigeminy with aberrant conduction. Why does aberrant
conduction ever occur? It is simply because the two bundle branches
(BBs) have different length of refractory periods. If an impulse
occurs when one BB is still refractory while the other has recovered from the
refractory period, the impulse will conduct thru the recovered BB, bypasssing
the refractory BB: aberrant conduction results. Of course, if an impulse occurs
at a time when both BBs have recovered from the refractory period, it will
conduct normally, while if both BBs are refractory, it won’t conduct at
all (non-conducted PAC). This was well diagrammed and explained in the
Medscape ECG of the week posted on 3/7/2012.