This case comes from Sam Ghali (@EM_RESUS). Thanks, Sam!
An 60-something male with h/o CABG presented with chest pain.
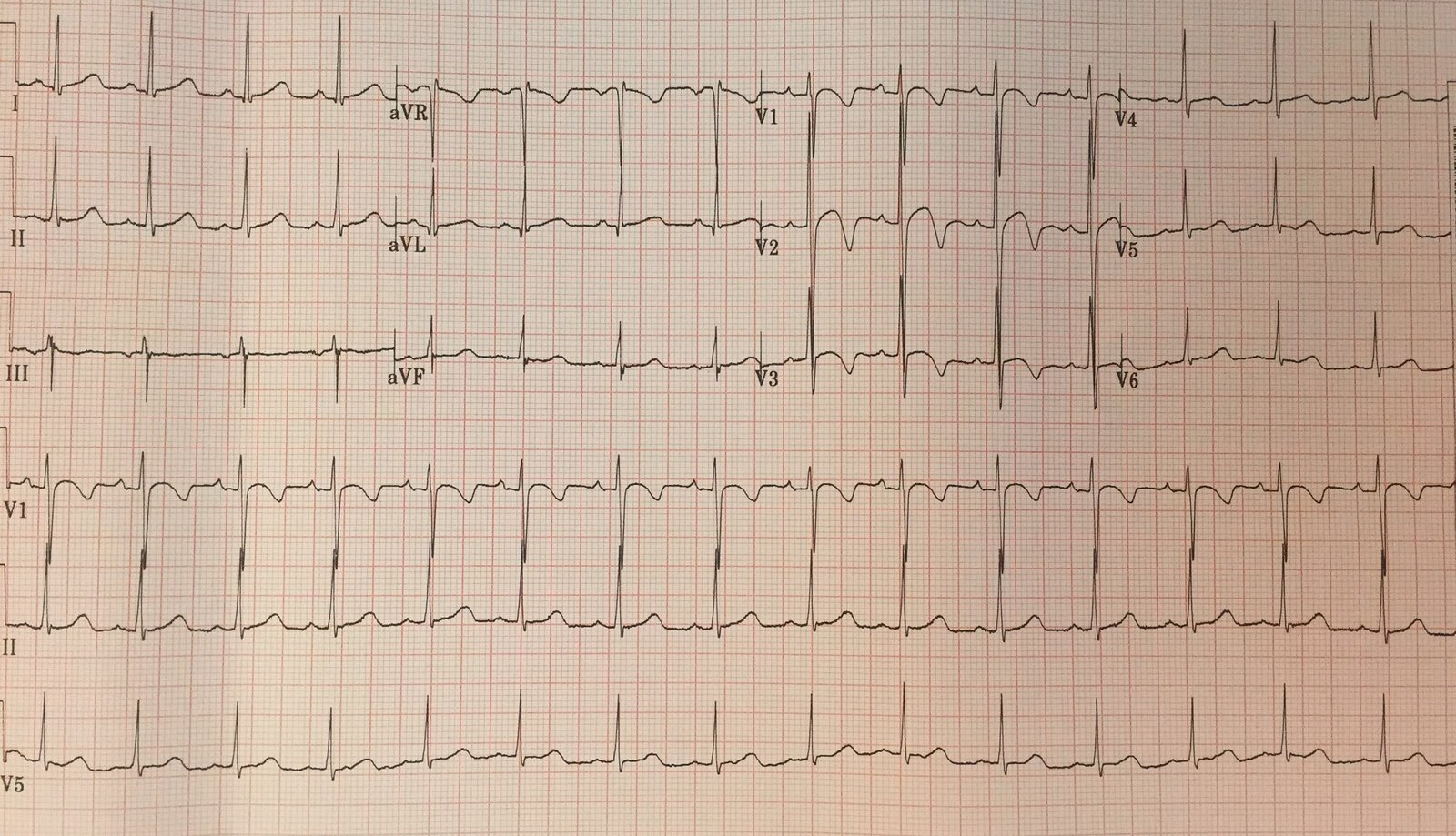
Here is his first ED ECG:
 |
| Sinus rhythm with PVCs. There is right bundle branch block and left anterior fascicular block (Often a bad combination!–see this post) There is ST elevation in V1-V3 and upright T-waves in V2, V3.RBBB should never have ST elevation. Anywhere. Especially in leads V1-V3, there is usually up to 1 mm of ST depression with an inverted T-wave. |
There is no ST elevation in I and aVL, so this is not a proximal LAD occlusion and thus the RBBB + LAFB is probably not due to the MI (it is likely old, pre-existing) and thus does not have the same terrible prognosis as acute RBBB + LAFB in proximal LAD occlusion)
Sam activated the cath lab.
There was a slight delay.
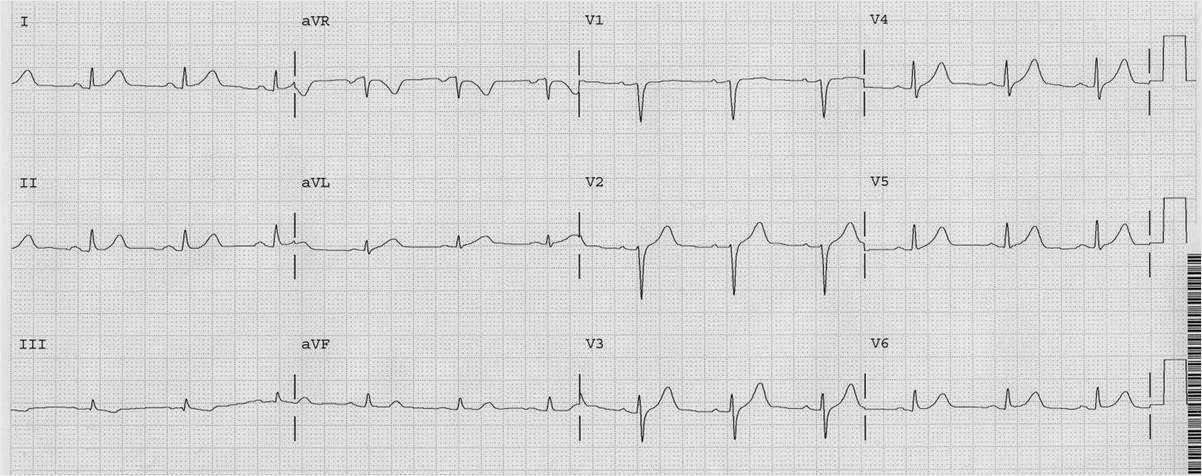
The patient suddenly felt better, and this ECG was recorded 19 minutes after the first:
 |
| Back to normal RBBB. (Now also left anterior fascicular block) This is just the way RBBB without ischemia should look: ST depression and T-wave inversion discordant to (opposite direction of) the R’-wave. This just confirms that the LAD was occluded and underwent spontaneous reperfusion (autolysis of thrombus). |
At angiogram, there was diffuse disease but no definite culprit identified. The patient was managed medically without a stent. Details are below for any who want to read them.
Unless thrombus is seen, it is very difficult to identify the culprit, though it often can be done with intravascular ultrasound (IVUS), which may identify ulcerated plaque. When there is diffuse severe CAD, this becomes very difficult.
In 5-10% of STEMI, the culprit cannot be identified.
Serial troponin T were: 0.026, 0.040, 0.049 (barely elevated).
Echo showed apical akinesis and EF of 50-55%.