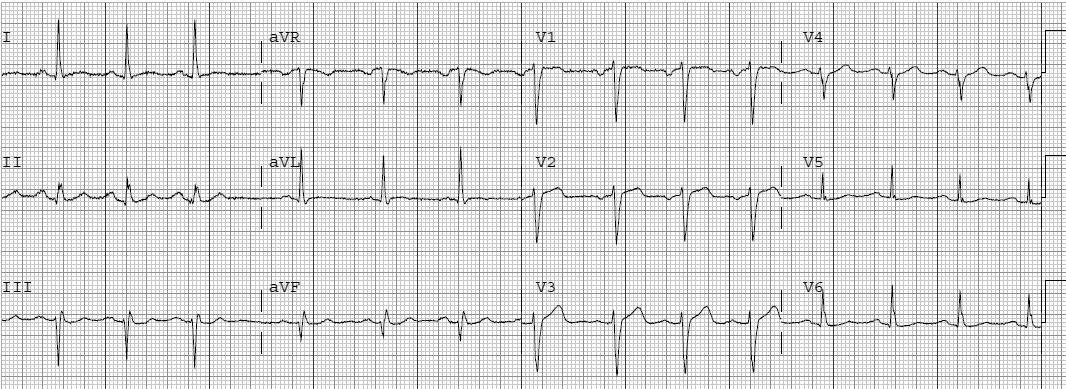
This 69 yo male with a history of HTN, but no h/o CAD, presented with chest pain at an outside hospital at 1700 hours with chest pain onset at approx 3 PM. Here is the first ECG, at 1720:
 |
| There is a negative T-wave in lead III, but this is not necessarily abnormal: the T-wave (18 degrees) and QRS (+9 degrees) axes are very close to each other. The negative T-wave in aVF also looks suspicious, especially since the QRS appears to be upright. Otherwise, the ECG is normal |
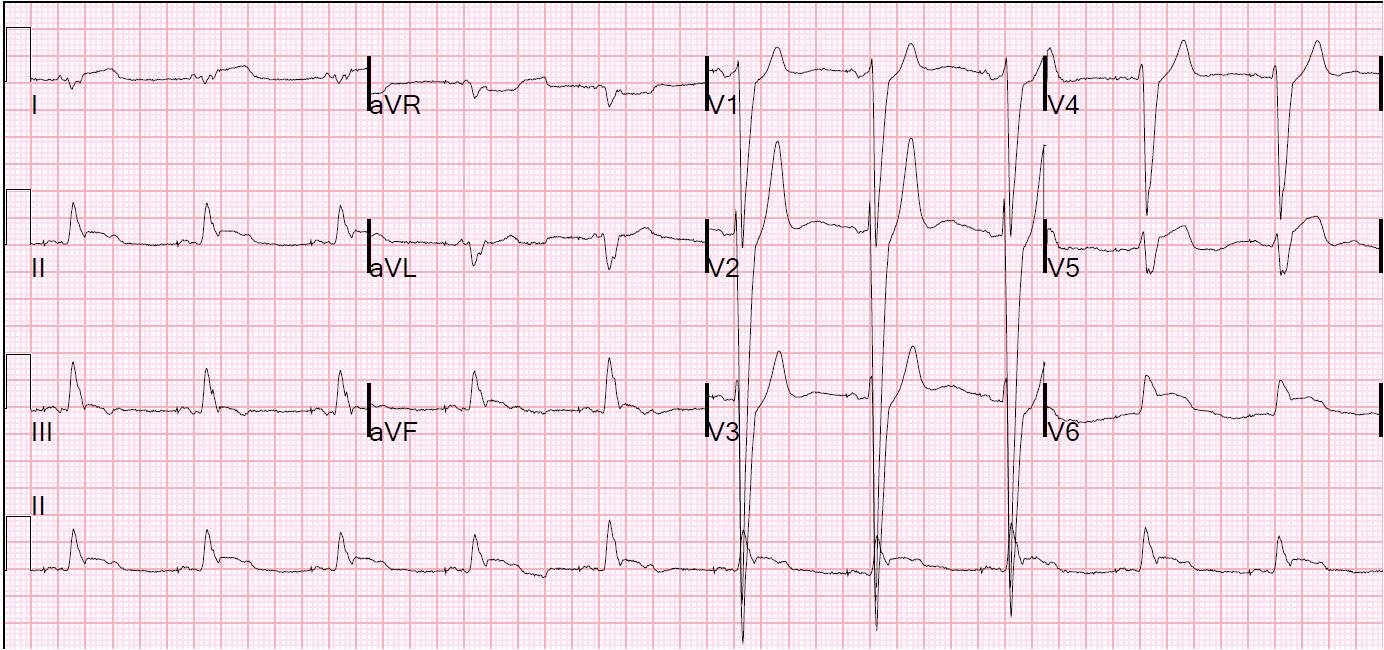
The patient received nitroglycerin, and became pain free. A second ECG was recorded at 1739:
 |
| Thanks to Christopher for noticing that the leads were switched from the previous ECG, with this ECG having correct lead placement. Now the inferior T-waves are upright because the leads are correctly placed and the axis is more normal. Nevertheless, there is now T-wave inversion in aVL. Additionally, ST depression can now be seen in leads V2 and V3, suggesting posterior MI. These highly suggest posterolateral MI, probably circumflex, with reperfusion due probably to nitroglycerin. |
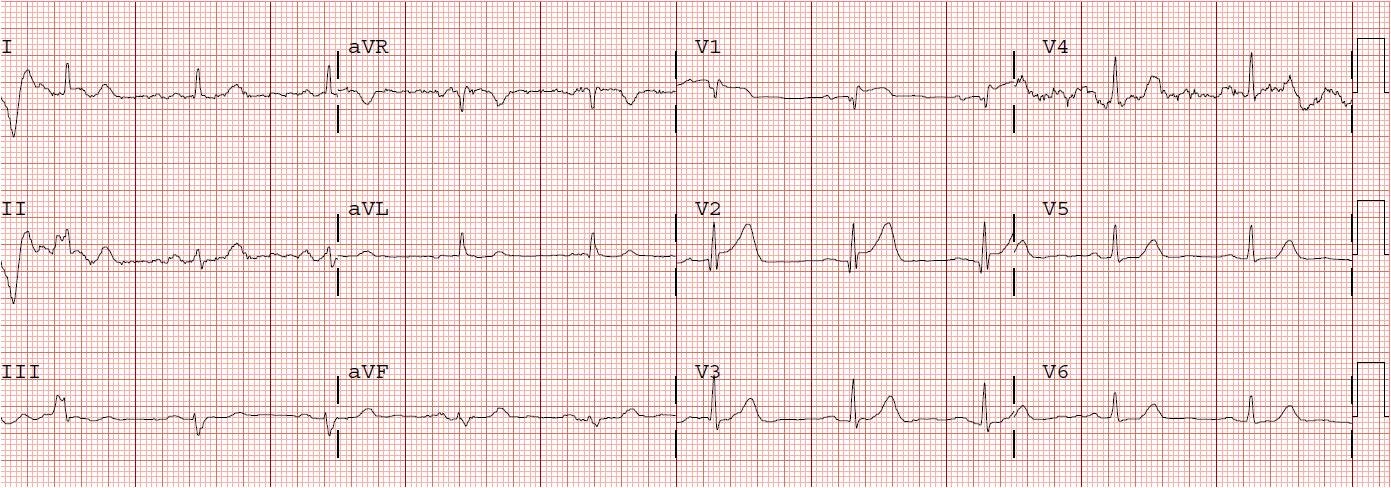
The patient was put on heparin and eptifibatide and transferred to our institution. Here, he remained pain free. His initial Troponin I was 16 ng/ml. A 3rd ECG was recorded at 2202:
 |
||
| The ST depression in precordial leads is gone. The biphasic T-wave in aVL remains, with an abnormal reciprocal ST segment in lead III. |
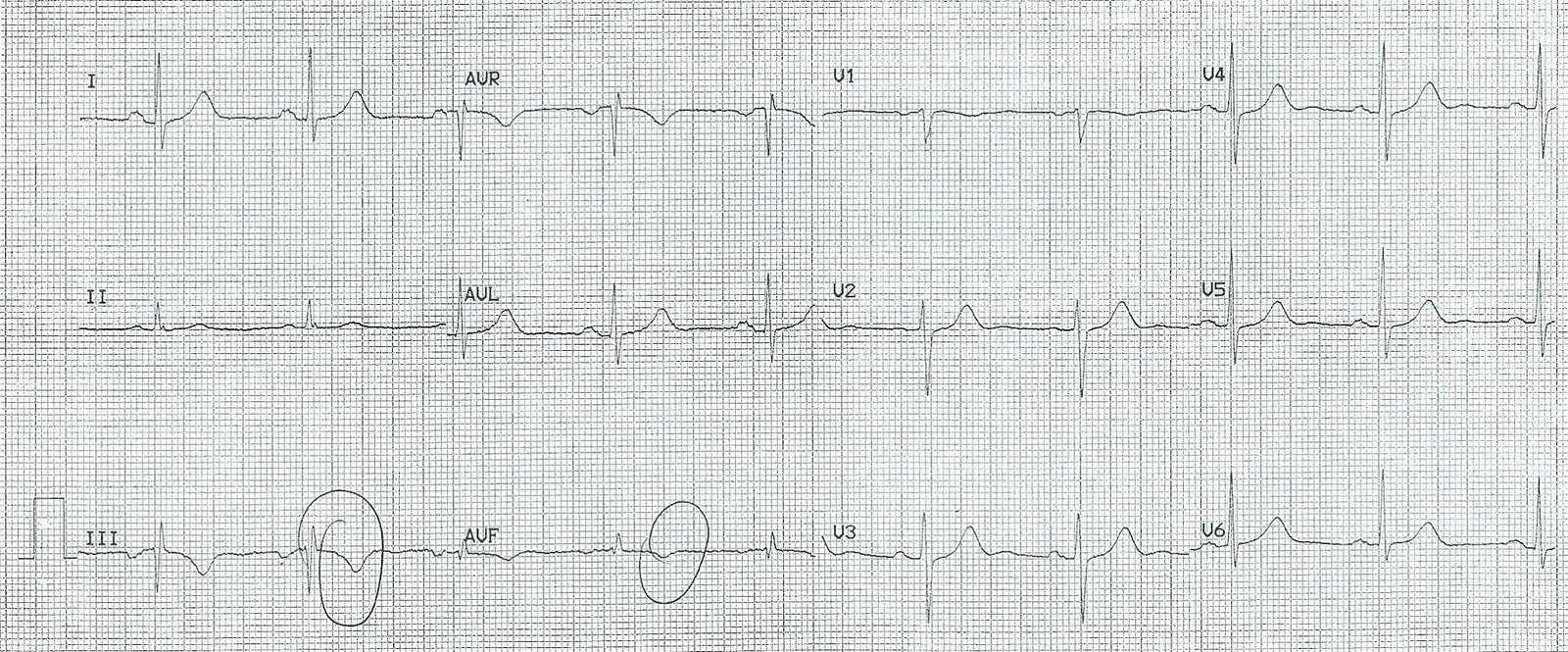
At 0032 another ECG was recorded:
 |
| This shows enlarged T-waves in V2-V3, an example of a heretofore never described (except on this ECG blog) phenomenon of what I call “posterior reperfusion T-waves.” Reperfusion T-waves are inverted, but if one makes an anterior (precordial) recording of inverted posterior reperfusion T-waves, then one gets enlarged anterior T-waves. |
Here is another example of posterior reperfusion T-waves:
https://drsmithsecgblog.com/2010/12/computer-misses-again-two-cases-one.html
The next AM the patient went into atrial fib with RVR:
 |
| The tachycardia has resulted in recurrent ischemia. Now there is ST elevation in aVL (and reciprocal ST depression in lead III) and ST depression in precordial leads (posterior subepicardial ischemia). |
He was taken for cath and had a 100% occlusion of a large 1st obtuse marginal (circumflex). Ultrasound confirmed a posterolateral wall motion abnormality. The troponin peaked at 74, went down, then went back up to 180 after the atrial fib, and down again.