This is complementary to a recent previous post.
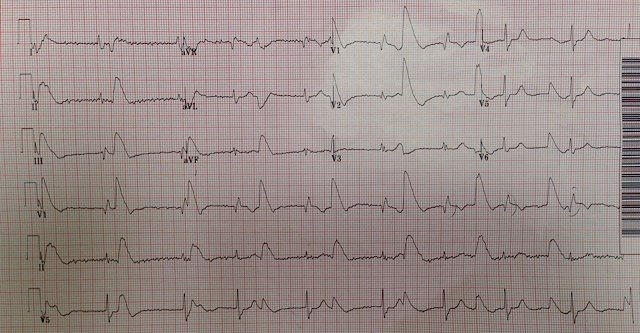
A dialysis patient presented with pedal edema. As a screen for hyperkalemia, an ECG was recorded:
 |
| QRS duration is 183 ms. What do you think? |
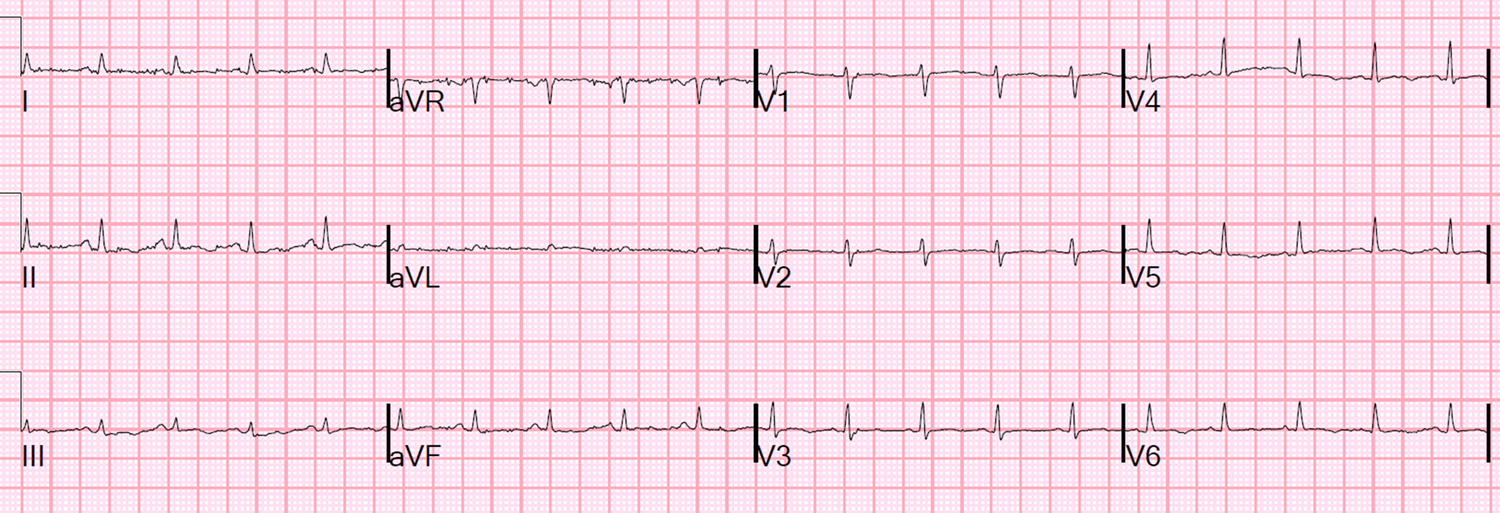
A previous ECG was immediately found at a time when the K was 6.1 mEq/L:
 |
| QRS duration is 167 ms, but a previous ECG with a normal K had a QRS of 184 ms. What do you think? |
This shows how subtle hyperkalemia can be, and yet still be diagnostic.
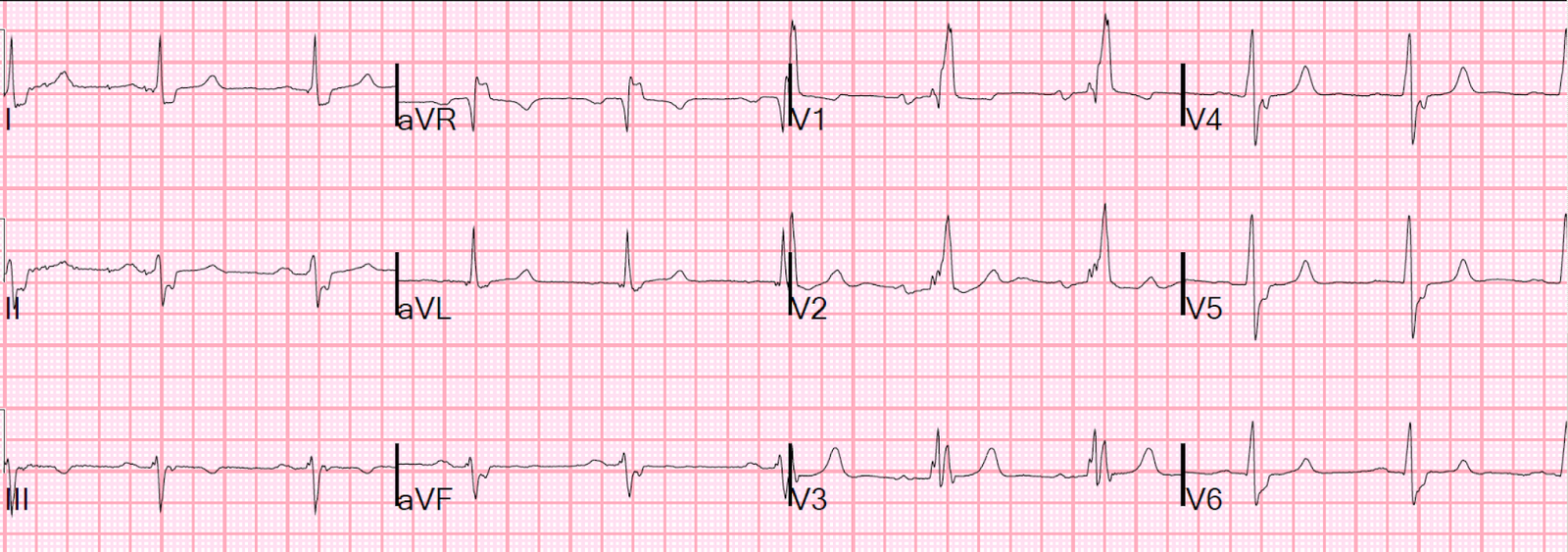
See the two side-by-side here:
Previous, with K 6.0 mEq/L This Visit
 |
| Notice how the ST segment is flatter on the right than on the left (see especially lead V4). Such a flat ST segment is part of what makes the T-wave peaked, as the rise of the T-wave from a flat ST segment is very steep. |
In RBBB, a QRS duration greater than 175 ms should make you strongly suspect hyperK (see this link!). In this case, in the past, there actually had been such a long QRS in the presence of a normal K, so this case was an exception.
The patient’s K was 7.1 mEq/L.