This is a repost of part of one of the most viewed posts ever.
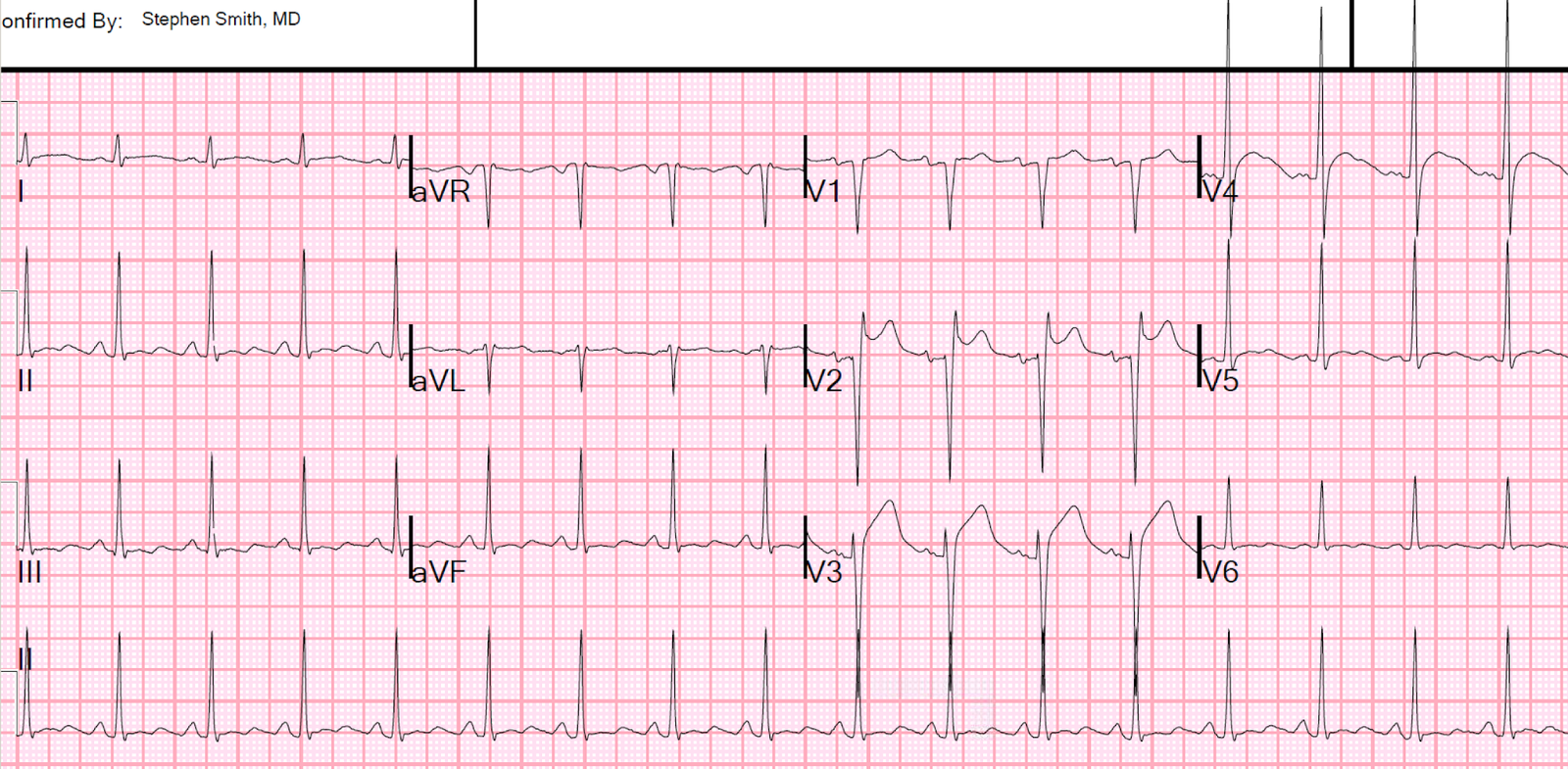
This patient with little past medical history presented feeling moderately ill. He had an ECG recorded:
 |
| QRS duration = 102 ms. What do you think? |
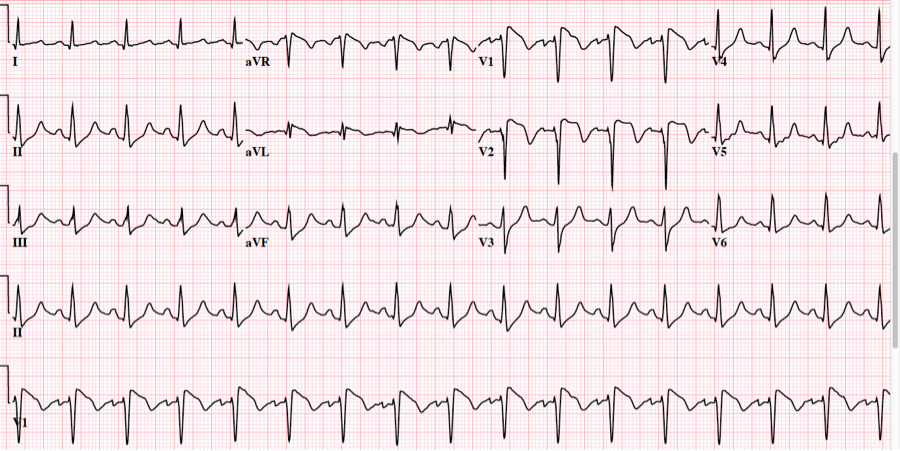
Due to the peaked T-waves, the residents were immediately concerned for hyperkalemia and sought an old ECG, which they immediately found in the medical record. It was recorded with a K of 4.5 mEq/L:
 |
| QRS 82 ms. |
The residents interpretation was that these were identical. After viewing this previous ECG, and knowing that the K was 4.5 at the time it was recorded, the residents believed that the peaked T waves in ECG #1 were this patient’s baseline.
Are they identical?
Inspect lead V4 more closely, here for a side by side comparison:
 |
| On the left, the ST segment is nearly flat and rises abruptly. On the right, it is not flat (though nearly so) and rises slightly less abruptly |
It is true that early repolarization has tall and relatively peaked T waves, but not to the extent seen in ECG #1. Without seeing them side by side, it is hard to appreciate the difference.
This patient, then, did not get immediate treatment for hyperK.
I saw these ECGs at a slightly later time than the resident, recognized the difference and, worried about the patient, started toward his bedside. As I was approaching the patient, he had a v fib arrest. He was immediately resuscitated, then his K returned at 7.0 mEq/L. This was a presumed hyperkalemic arrest.
Some say you don’t need to treat hyperK unless there is QRS widening. They claim that peaked T-waves are not enough. This is only one case, and anecdotal, but we found no other etiology of arrest in this patient. I always treat immediately if the ECG is affected by hyperK.
There is a definite difference, with EKG 1 pathognomonic for hyperkalemia.