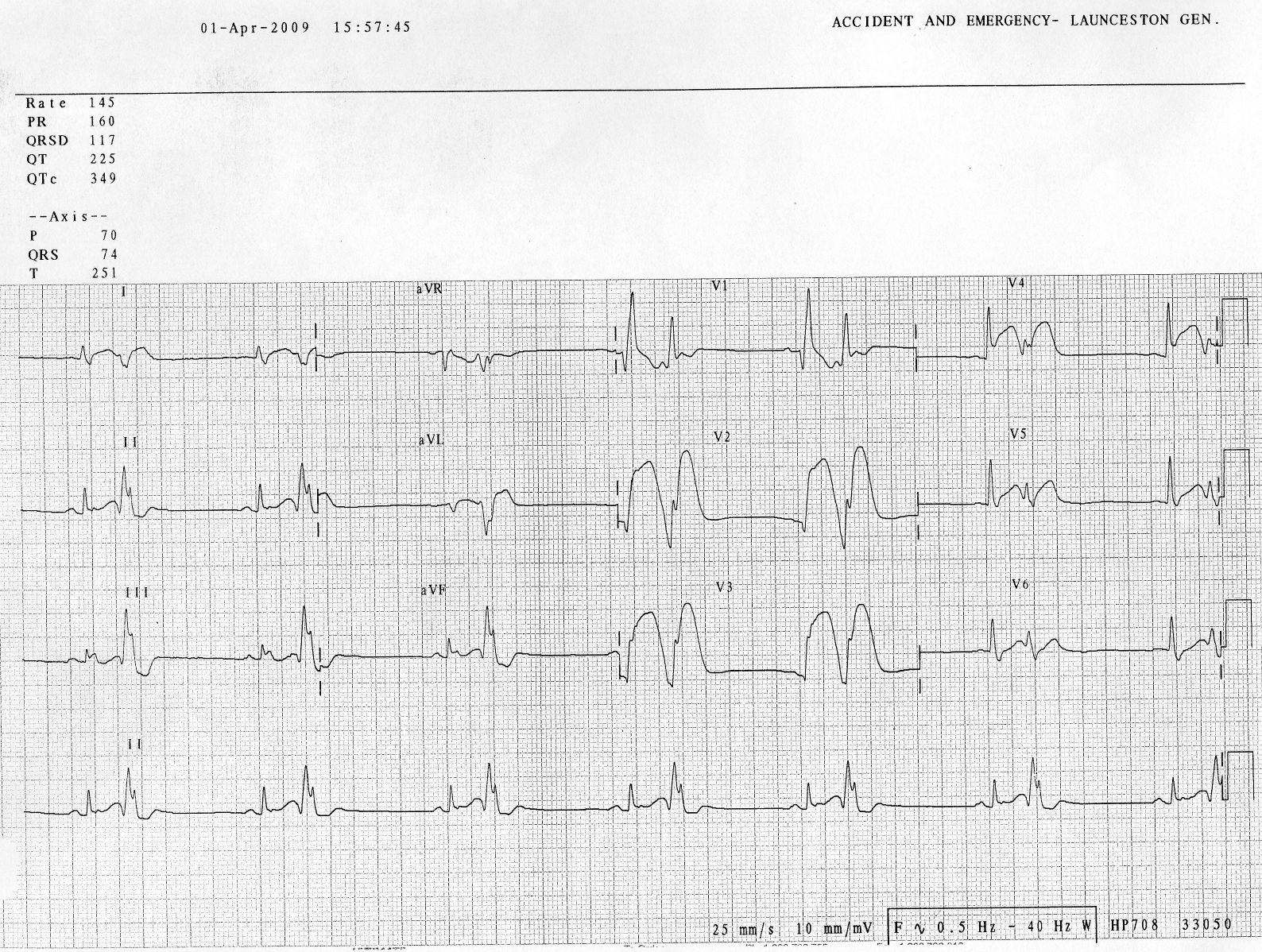
This patient is 38 years old with hyperlipidemia. He was at the gym when he had the onset of chest pain. EMS was activated and recorded the following ECG (scanned from a prehospital ECG, so the quality is not perfect):
Notice the small Q wave in V1 followed by a very large R-wave, with a prolonged QRS. There is a wide S-wave in V6. Thus, there is right bundle branch block, which should never (unlike Left BBB) have any ST elevation. But here there is a large degree of ST elevation in V2-V6, I, and aVL. RBBB in acute STEMI has a very high mortality.
The paramedics activated the cath lab from the field.
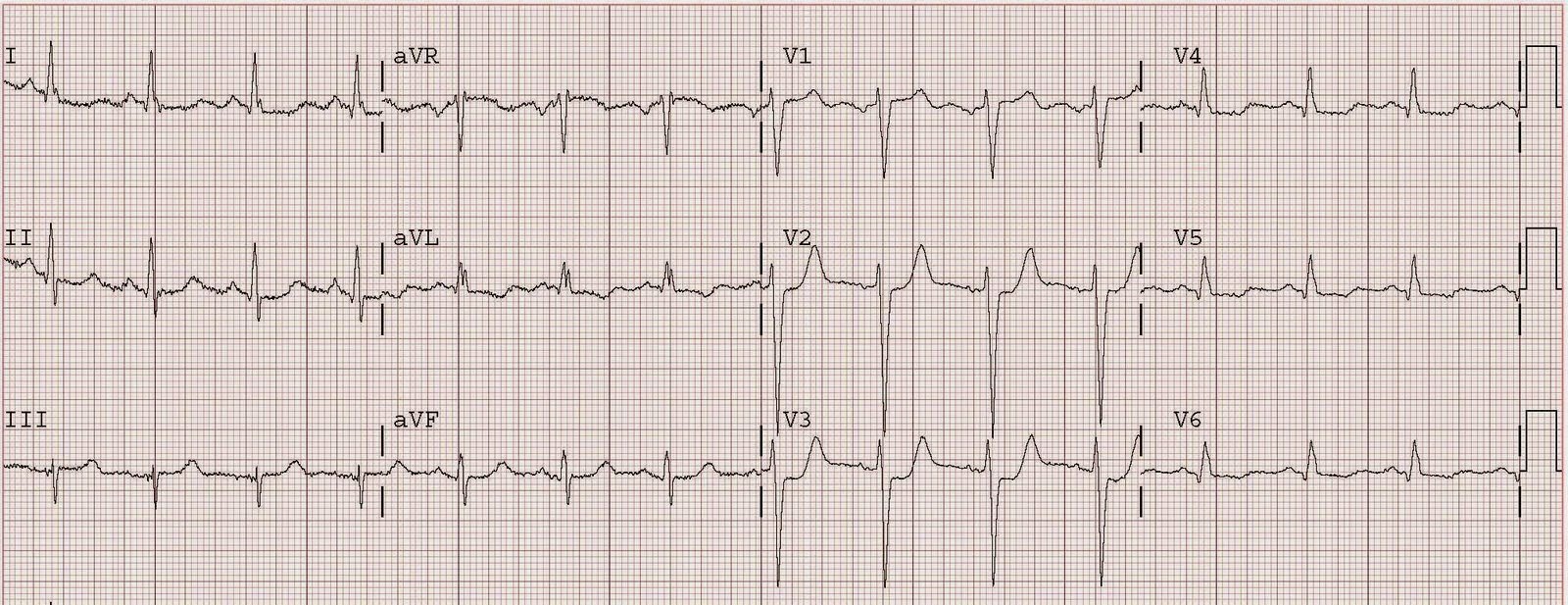
The patient had 2 ventricular fibrillation arrests during transport, but was immediately defibrillated both times, and was awake in the ED, when the following ECG was recorded:

The ST elevation has mostly resolved on this ECG, and were it not for the arrest and the prehospital ECG, this would not be a slam dunk diagnosis. There is still ST elevation in I and aVL, but it is subtle. There are abnormal T waves in V2-V4, with straightening of the ST segment which is typical of hyperacute T waves.
Angiography revealed a very tight LAD stenosis with some flow (confirming the reperfusion that we see on the ECG). A stent was placed, and the patient had an excellent outcome with no wall motion abnormality.
Learning point: the prehospital ECG is critical, as was early prehospital cath lab activation. Were it not for this prehospital ECG and the cardiac arrest, the diagnosis may have been significantly delayed. Had this happened, the artery may have re-occluded prior to angiography, with resultant recurrent cardiac arrest and/or shock and death.