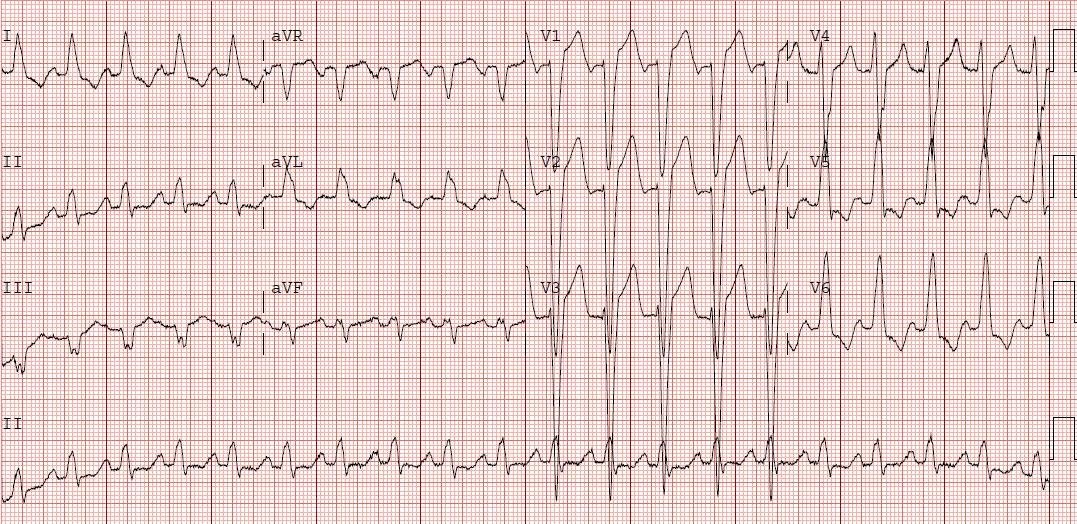
An 81 yo woman presented at 2 AM to the ED with severe substernal chest pressure. This ECG was recorded:
There is sinus rhythm with a PVC, and Right Bundle Branch Block (RBBB). Normally there is no ST elevation with RBBB. In fact, normally, there are inverted T waves (discordant to a positive QRS due to the large R’ wave, of the rSR’) and from 0-1 mm of ST depression. Any ST elevation in V2 or V3 is very suspicious for LAD occlusion in a patient with chest pain.
The cath lab was activated, but the interventionalist disagreed with the interpretation. A stat echocardiogram revealed anterior wall motion abnormality and the patient was taken for angiography which revealed a 95% ostial thrombotic LAD lesion. She went for immediate coronary bypass surgery.
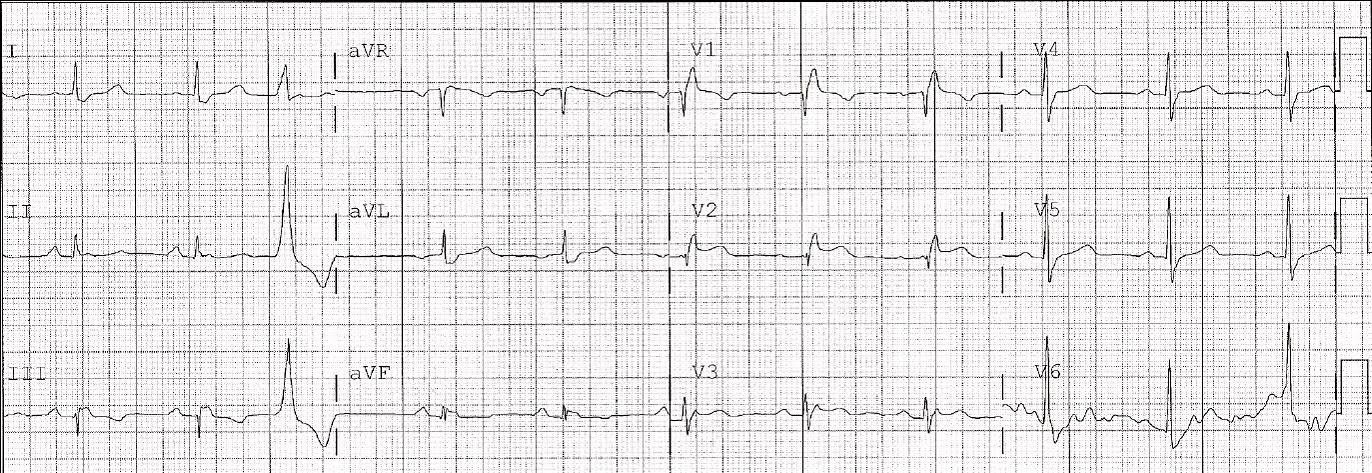
A similar case was posted on January 12, 2010. You can search for all the RBBB in the search box, or any of a great number of search terms to find other ECGs