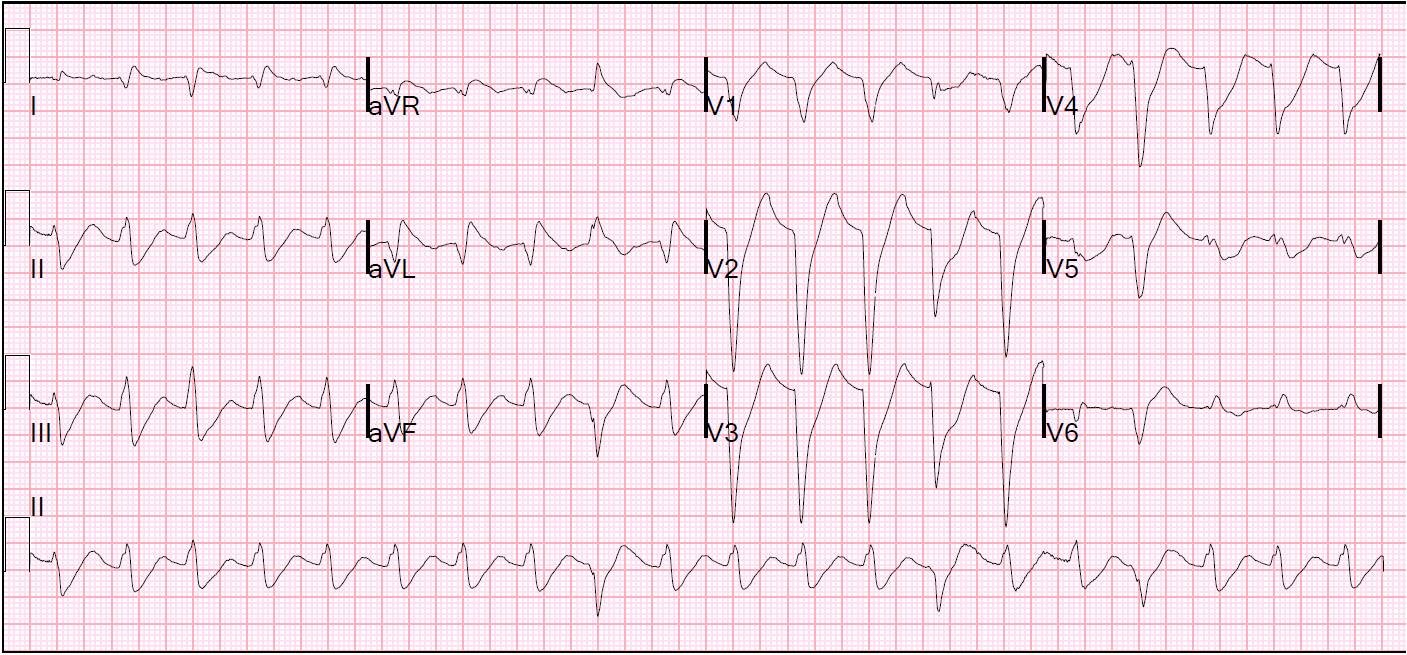
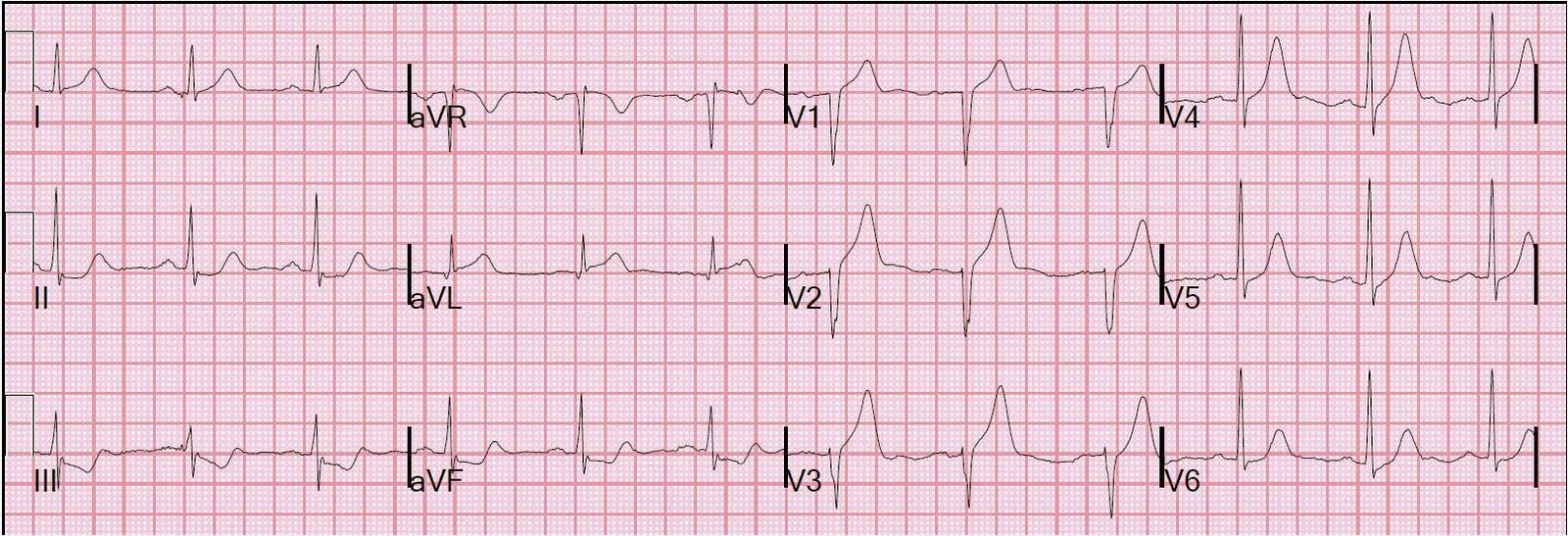
Chest pain and Right Bundle Branch Block
A 62 yo male with h/o CAD and stent in 1st OM presented with Chest pain while biking. Vitals were normal. An ECG was recorded: What do you…
Associate Editors:
— Pendell Meyers & Ken Grauer (2018)
— Jesse McLaren & Emre Aslanger (2022)
— Willy Frick (2024) — Sam Ghali (2025)