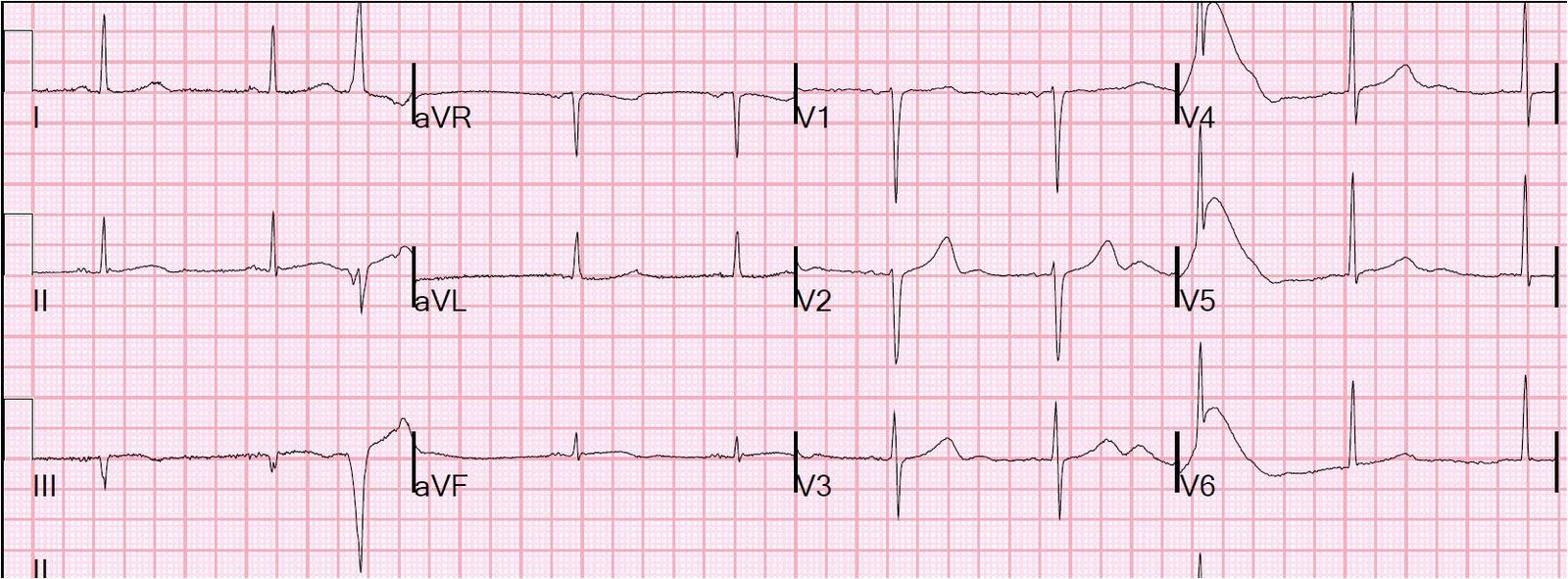
This is a 34 yo female with no history of CAD who had the onset of chest pain at 0900. It was constant, achy, substernal, 7/10, non-radiating, aggravated by smoking and movement and relieved with short deep breaths. She took analgesics without relief. She had had an episode one week prior. She smokes 2 packs per day and has a family history of early CAD. She has diet controlled DM. She presented at 1930 and had this ECG recorded:
 |
| There is just under 1 mm of ST elevation in I and aVL, with reciprocal ST depression in inferior leads, especially III. This should alert you to the high probability of lateral MI. This STE is more pronounced than in this case which was a false positive, posted a few days ago. Notice also that there is less than 1 mm of ST depression in V1-V3. This is highly suspicious for concomitant posterior MI, and should raise your index of suspicion very high because lateral MI is frequently accompanied by posterior MI when the circumflex artery is involved. |
The clinicians did not appreciate these findings. They administered aspirin and arranged for a telemetry bed. The patient continued to have pain and 2 more ECGs were recorded at 2145 and 2225, without any evolution. At 2059, the first troponin I returned at 14.19 ng/ml, confirming AMI of considerable duration. Apparently, the clinicians must have believed at first that it was a NonSTEMI because they waited until 2245 to activate the cath lab.
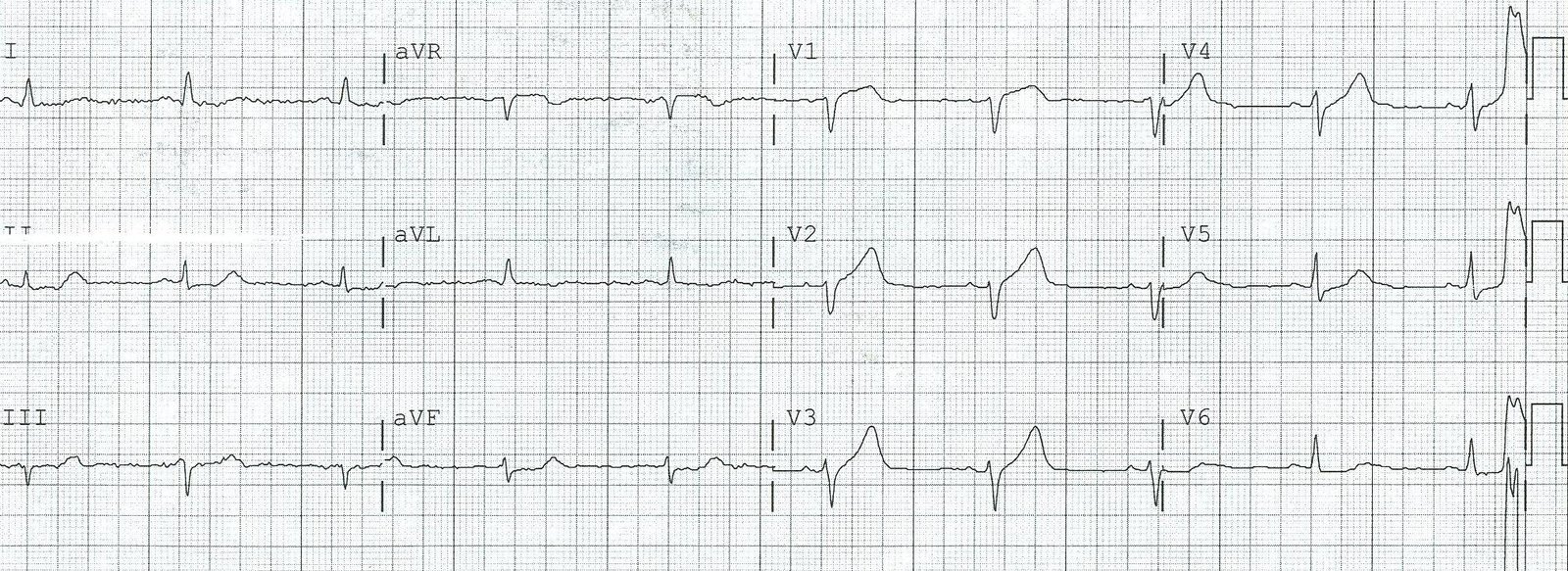
At cath, there was a 100% occluded proximal circumflex which was opened and stented. The troponin peaked at 300! (very large MI). Echo the next day showed a posterolateral wall motion abnormality and an ejection fraction of 40%. Here is the post cath ECG:
 |
| ST segments have resolved, confirming good microvascular reperfusion. |
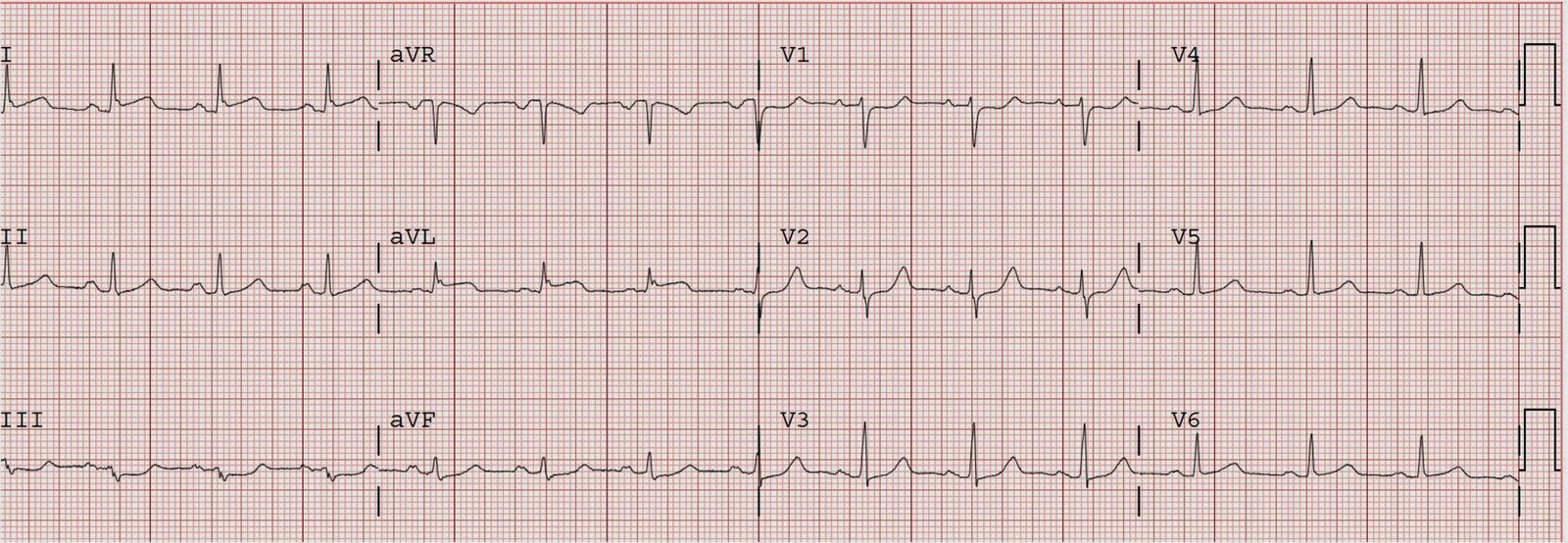
One week later, this was recorded:
 |
| Now there are clearly inverted T-waves in I and aVL (lateral reperfusion T-waves). If there were posterior leads, the T-waves would be inverted, but since they are recorded in anterior leads, we see instead a phenomenon that I call “posterior reperfusion T-waves”–the T-wave which would appear inverted on posterior leads appears larger on anterior leads. |
Learning point: Lateral MI may be very large but electrocardiographically subtle. Inferior ST depression is nearly always seen in lateral MI. Concomitant right precordial (V1-V3) ST depression makes the case for lateral MI, as the posterior wall is often supplied by the circumflex.