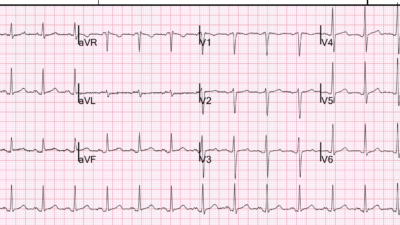
Case 1. A middle-aged woman presented with severe substernal crushing chest pain radiating to the left shoulder. This was her presenting ECG:
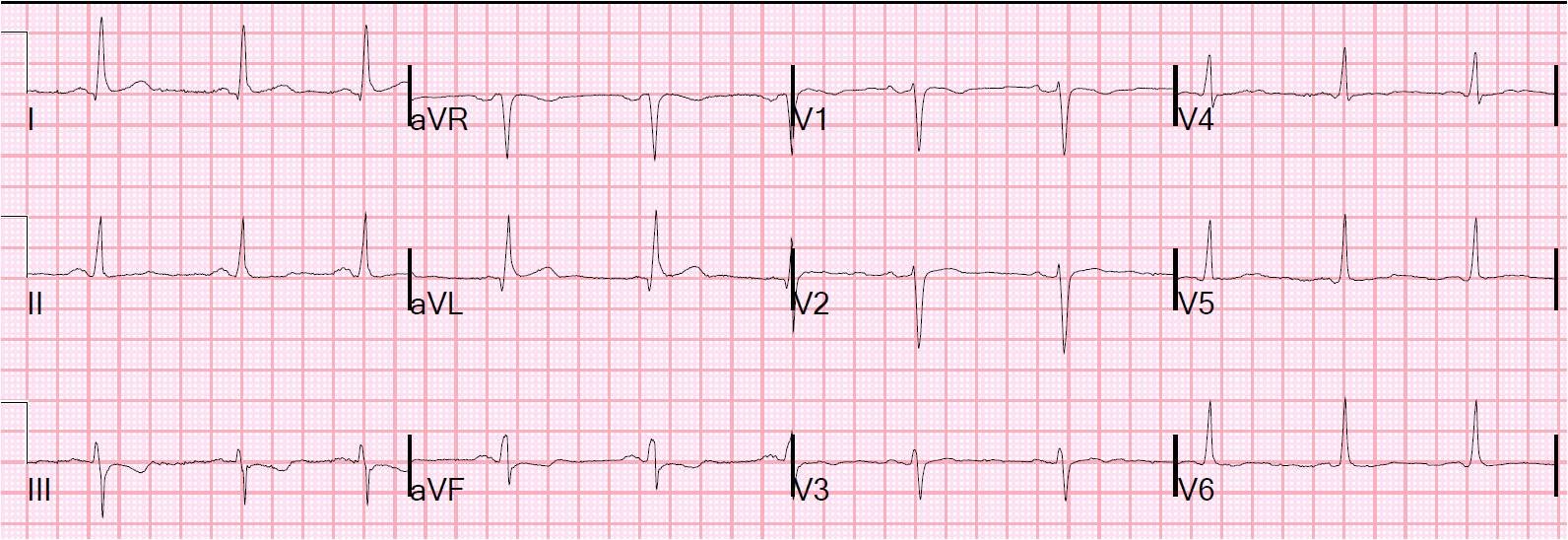 |
| There is a Q-wave in aVL and Minimal ST elevation in I and aVL (less than 0.5 mm) in the context of a 10 mm QRS. There is minimal reciprocal ST depression in III. There are some features of left anterior fascicular block, but there is not enough left axis deviation to meet criteria for this. This could be high lateral MI with circumflex or diagonal occlusion. |
Management options are to get an immediate echocardiogram, look for old EKGs (there were none), do serial ECGs, or just do an immediate angiogram. The interventionalist was consulted and he opted to go for immediate cath. It was negative.
Below are 3 typical cases (cases 2-4) of lateral ST elevation with inferior reciprocal ST depression that were actually circumflex or diagonal occlusions. In these cases, the findings are not as subtle as in case 1. But when you look at the last case (case 5), you’ll see how subtle real occlusion can be.
It is important to remember that only about 50% of lateral MI due to coronary occlusion have significant ST elevation, and for this reason the lateral wall is often called “electrocardiographically silent.” Often this is due to low QRS voltage in lateral leads, and because ST elevation is always proportional to the QRS, the ST eleavtion is low voltage. (See Schmitt et al. Chest 2001;120(5):1540-6, free full text)
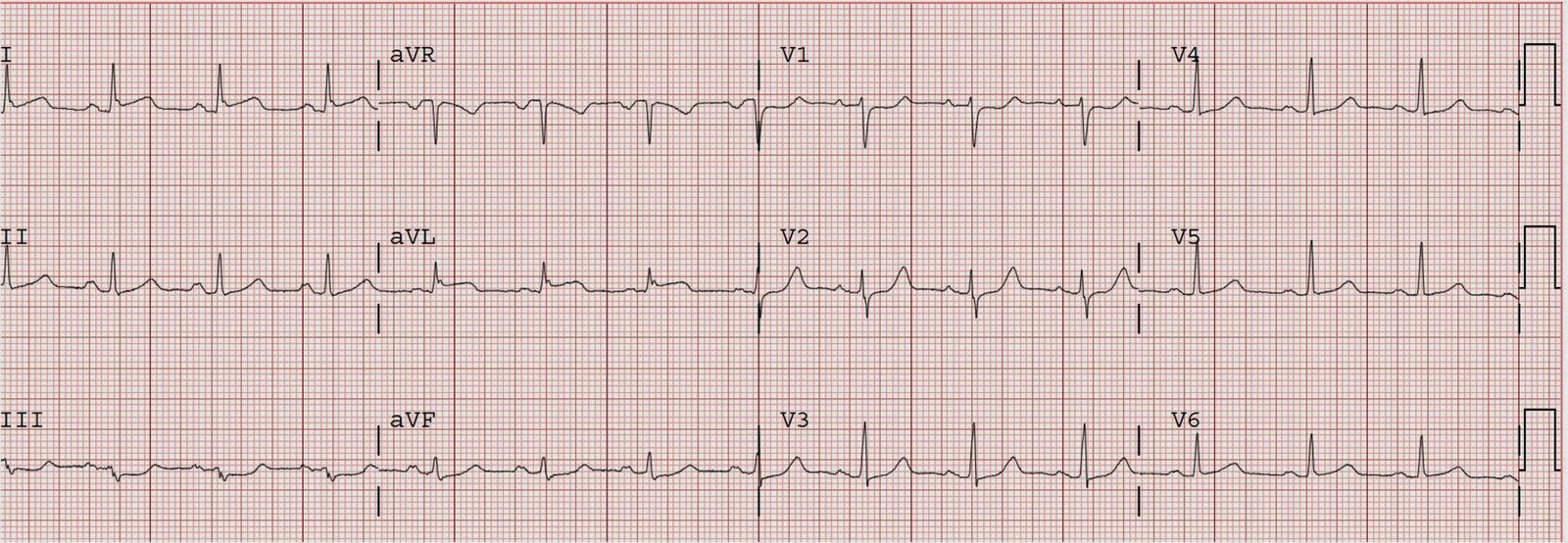
Case 2.
 |
| Acute Circumflex occlusion (also old inferior MI with Q-waves, and early repol giving anterior STE) |
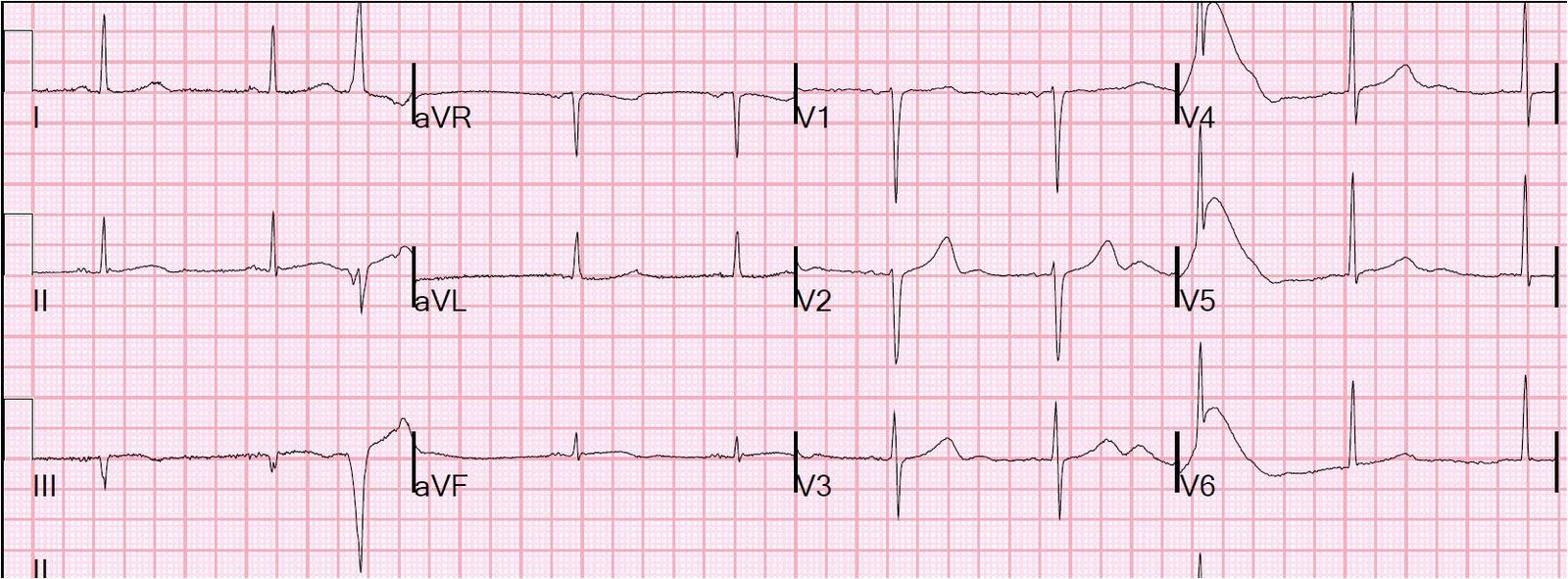
Case 3.
 |
| Lateral STEMI with very low voltage QRS in aVL, therefore very low voltage STE in aVL, but best seen by marked ST depression in inferior leads. Diagonal occlusion. Remember ST depression in inferior leads is not inferior ischemia, but rather reciprocal to lateral STEMI |
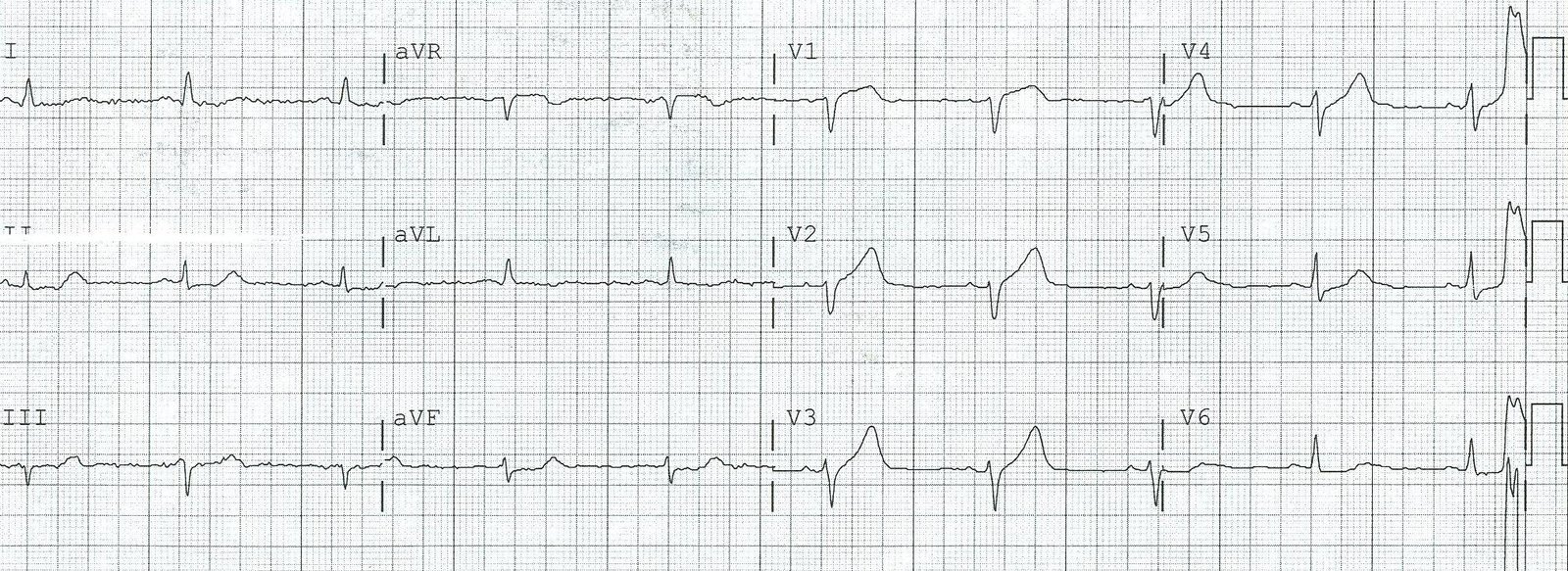
Case 4.
 |
| Circumflex occlusion with hyperacute T wave in aVL and reciprocal inferior ST depression. Notice the precordial ST depression of concomitant posterior STEMI. |
Case 5a.
 |
| D2 occlusion, lateral MI |
Case 5b.
 |
| After nitroglycerine, inferior ST depression and STE in aVL resolve. D2 is open by the time of angiography. |
Here is one of the most popular posts of all time, also relevant to this: ST depression does not localize: 2 cases of “inferior” ST depression of high lateral STEMI.