911 was called for an 18 year old who had altered mental status after using K2 (a recreational drug). The medics put the patient on the monitor and saw ST elevation. They then recorded a prehospital 12-lead (not shown, as it is identical to the ED ECG), which showed marked ST Elevation. The computer diagnosed “Pericarditis.” They were very worried, and brought the patient to the “Stabilization Room” for critically ill patients.
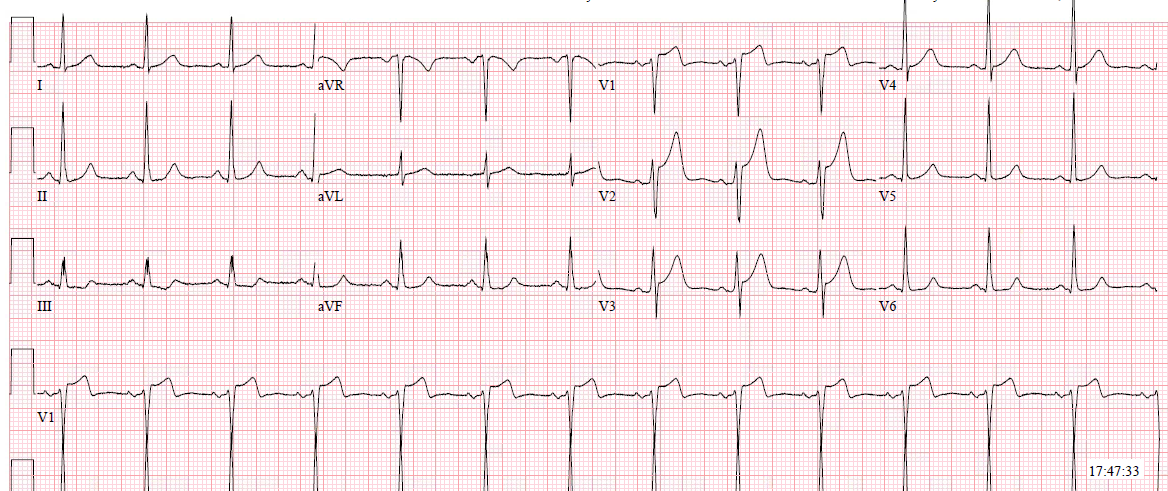
On arrival, I looked at the prehospital ECG (again, identical to the ED ECG shown below):
 |
| What did I think? |
I immediately said “Normal Variant ST Elevation,” and directed the patient to our “Special Care Unit” for altered mental status from drugs and alcohol.
This is not pericarditis, nor is it STEMI. Get to know this pattern just like you would get to know a friend. I called him “Jack,” and told the residents to get to know Jack.
Jack often has high voltage QRS, has marked J-waves (they look almost like Osborn waves). There is a relatively short QT interval. The ST Elevation is towards leads II and V5. Thus, there is no reciprocal ST depression in aVL. [In fact, these could be Osborn waves, but they were not: the patient was not hypothermic.]
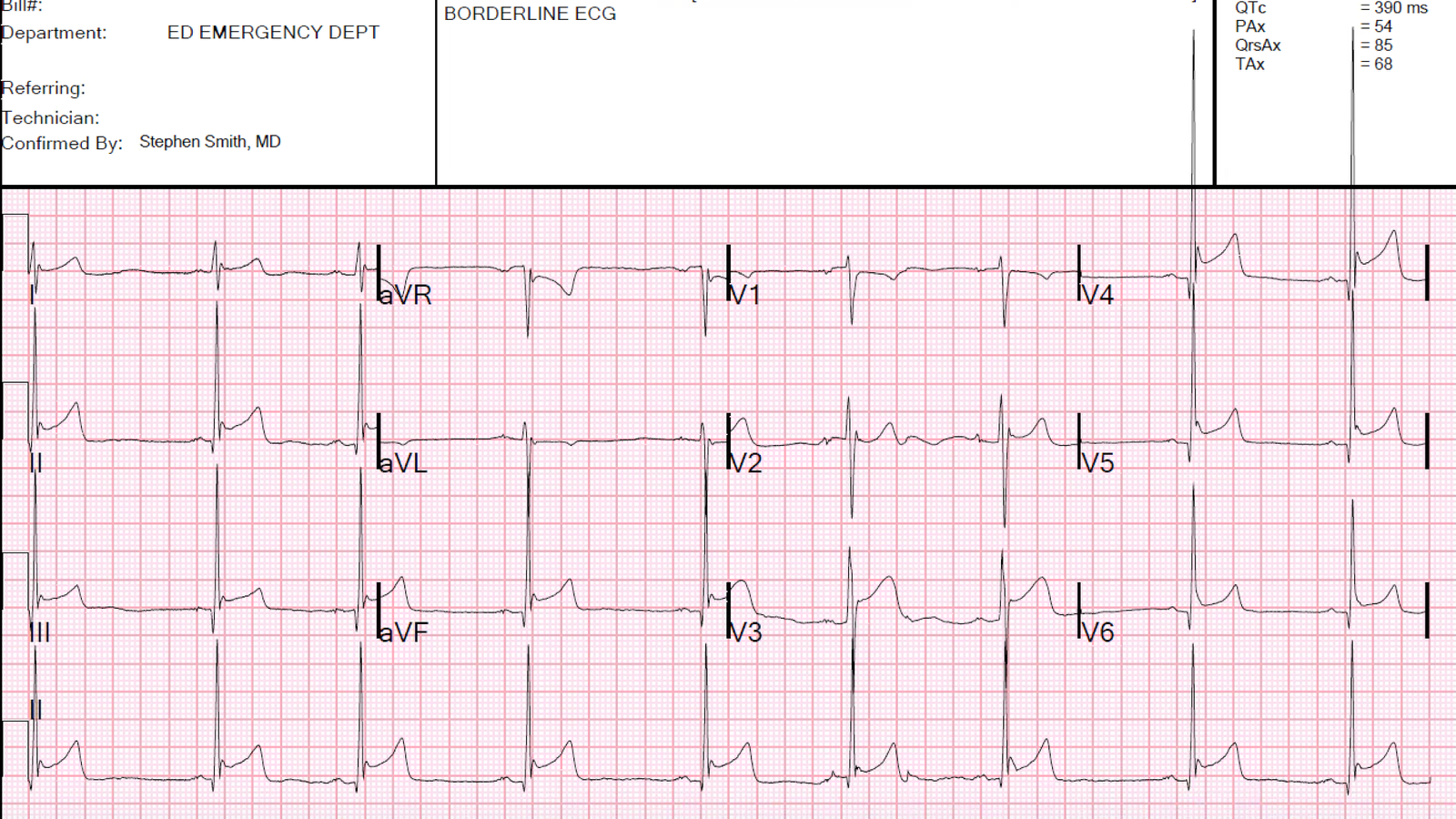
Although the T-wave is negative in aVL, it is NOT T-wave inversion, as the QRS-T angle is narrow (QRS axis is 85 degrees, almost directly inferior; T-wave axis is 68 degrees — angle is only 17 degrees. Both these measurements are accurately made by the computer algorithm.)
How do I know it is not pericarditis? First, the patient denied any chest pain! Second, normal variant STE is far more common that pericarditis. There are J-waves, no PR depression, and no Spodick’s sign (downsloping T-P segment — of questionable reliability).
It is very common for Normal Variant STE to be misdiagnosed as pericarditis. Does this have adverse consequences?? It may. Take a look at this case that was written by Pendell Meyers when he was a medical student: due to misdiagnosis of the ECG as “pericarditis”, a patient’s chest pain was misattributed to pericarditis and the correct diagnosis of pulmonary embolism was ignored: