As I have pointed out in other posts, I have developed an equation to help in the electrocardiographic differentiation of anterior early repolarization from anterior STEMI. If the equation [(1.196 x ST Elevation in mm at 60 ms after the J-point in V3) + (0.059 x computerized QTc) – (0.326 x R-wave Amplitude in mm in V4)] has a value greater than 23.4, vs. less than 23.4, it is quite sensitive and specific for LAD occlusion.
Remember: when you are uncertain, look for old ECGs, do serial ECGs, then, if you still need to, you can get an immediate echocardiogram, and if you ultimately cannot be certain that it is not STEMI, then you may have to risk a false positive cath lab activation. That happens.
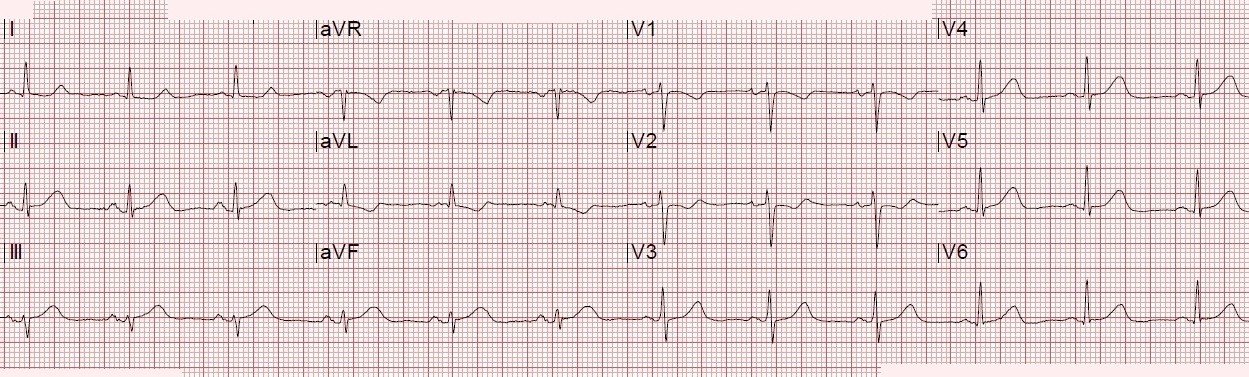
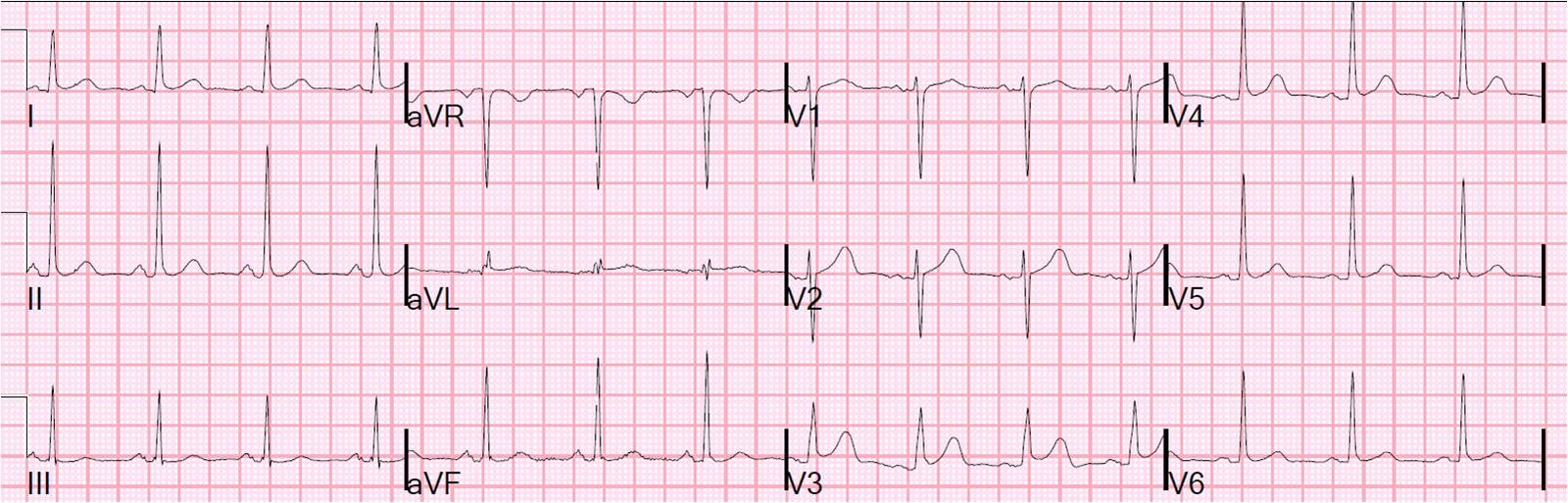
Case 1. One of my partners phoned me when I was out. He was worried about this ECG. He used his iPhone to photograph it, then sent it to me by text message:
 |
| Computerized QTc was 391 ms, STE at 60 ms after the J-point is 2 mm, R-wave is 11.5. I looked at it at said I do not think it is STEMI. If you apply the equation, the value is 21.7 (less than 23.4, so it is early repolarization). |
I told him that it is very unlikely to represent STEMI.
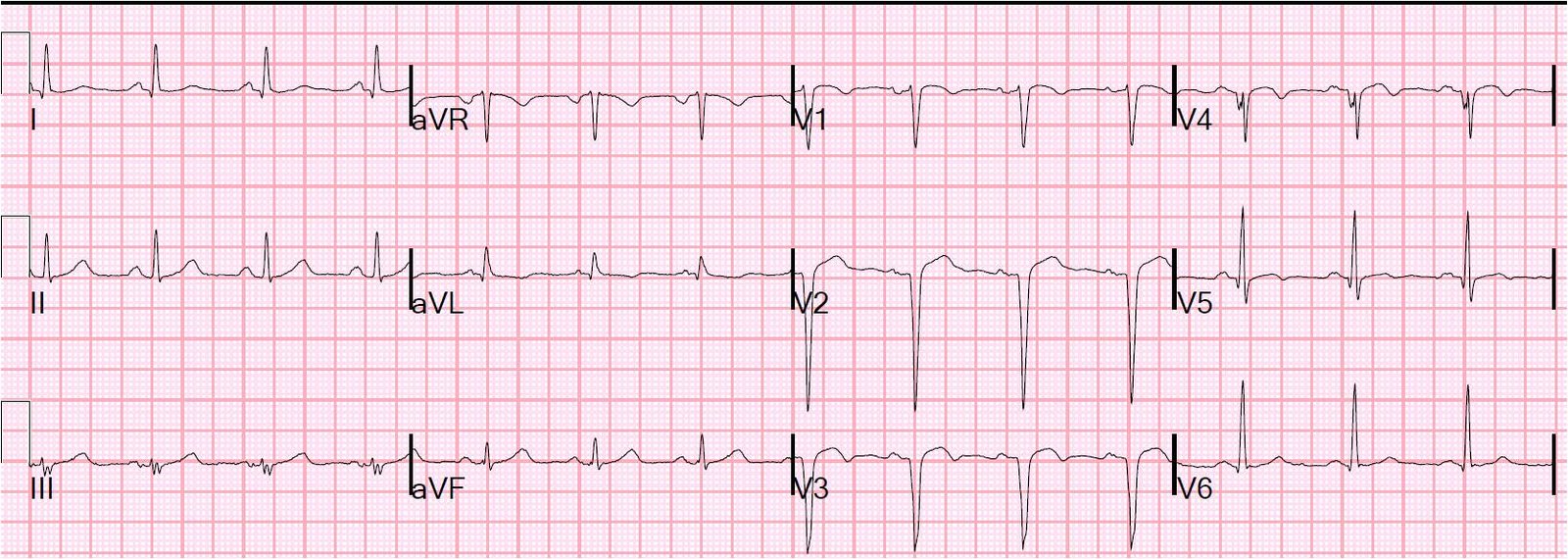
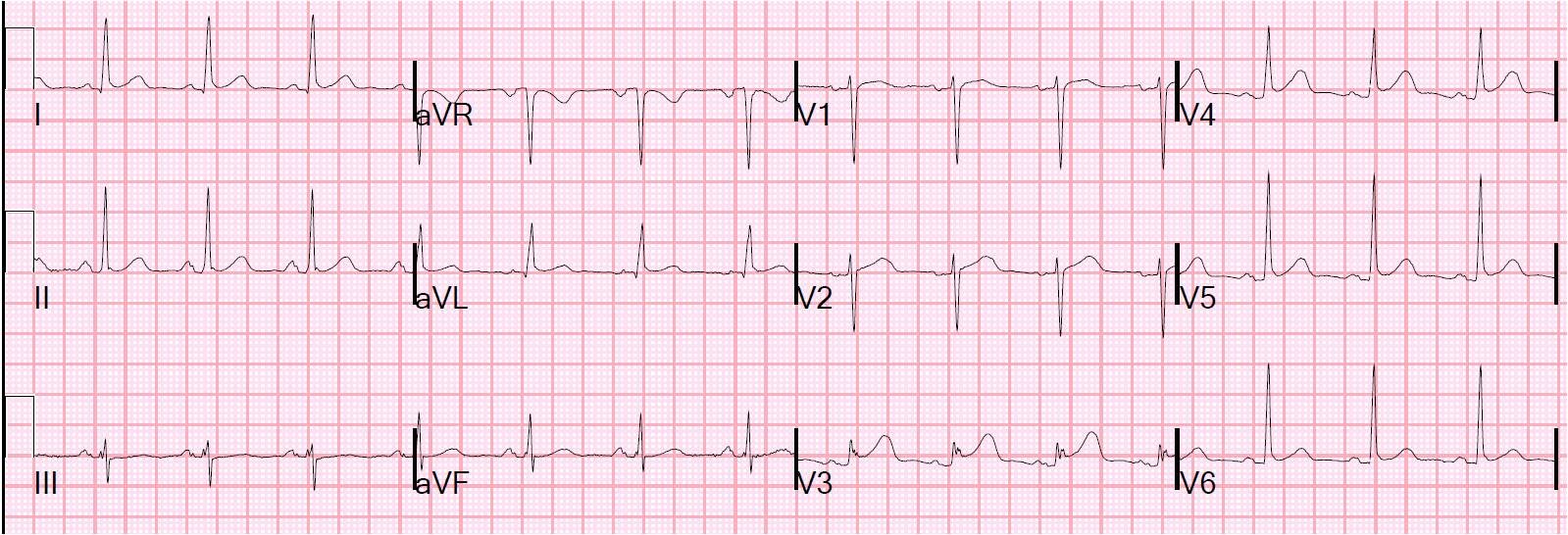
Here is a previous ECG from one year ago:
 |
| The new one looks different from this one, especially in V3, but this can happen in early repol |
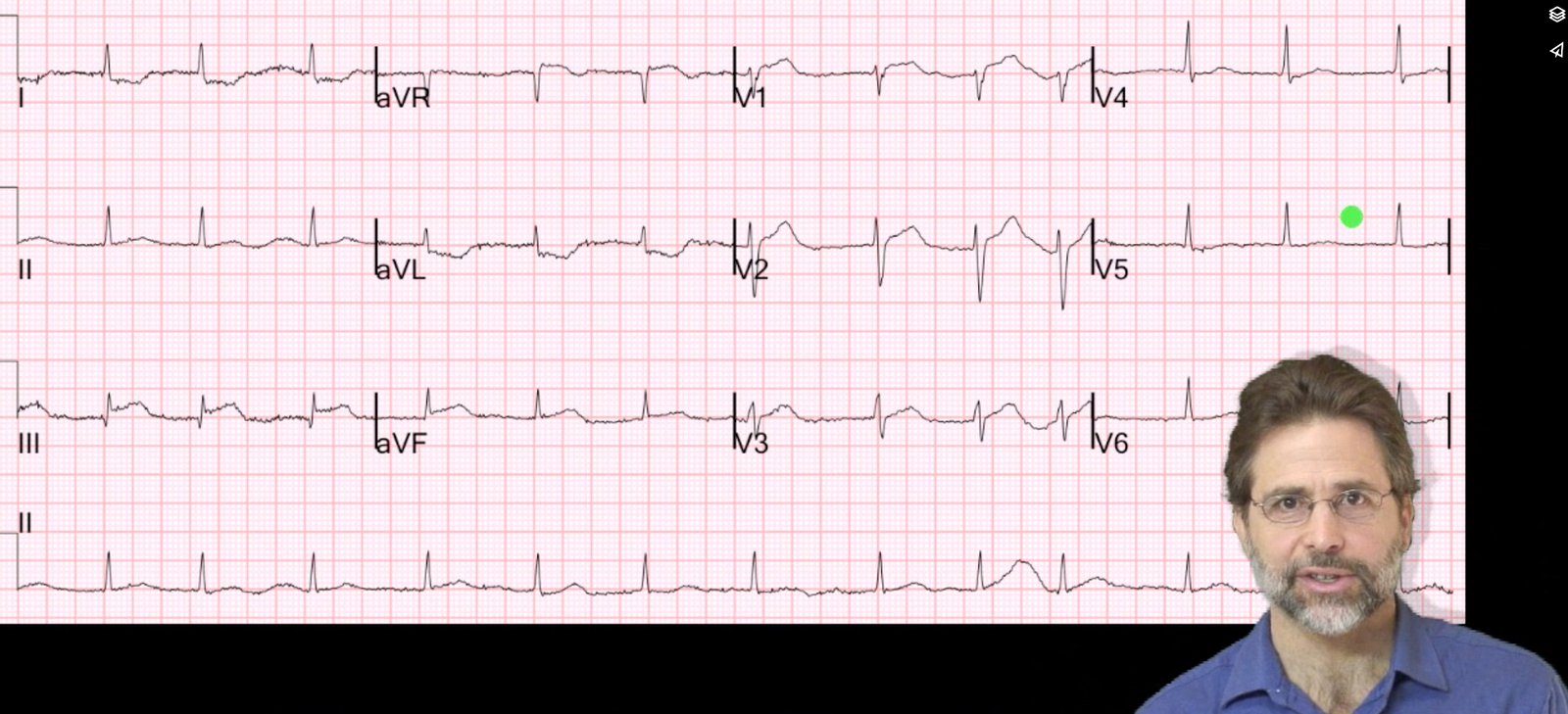
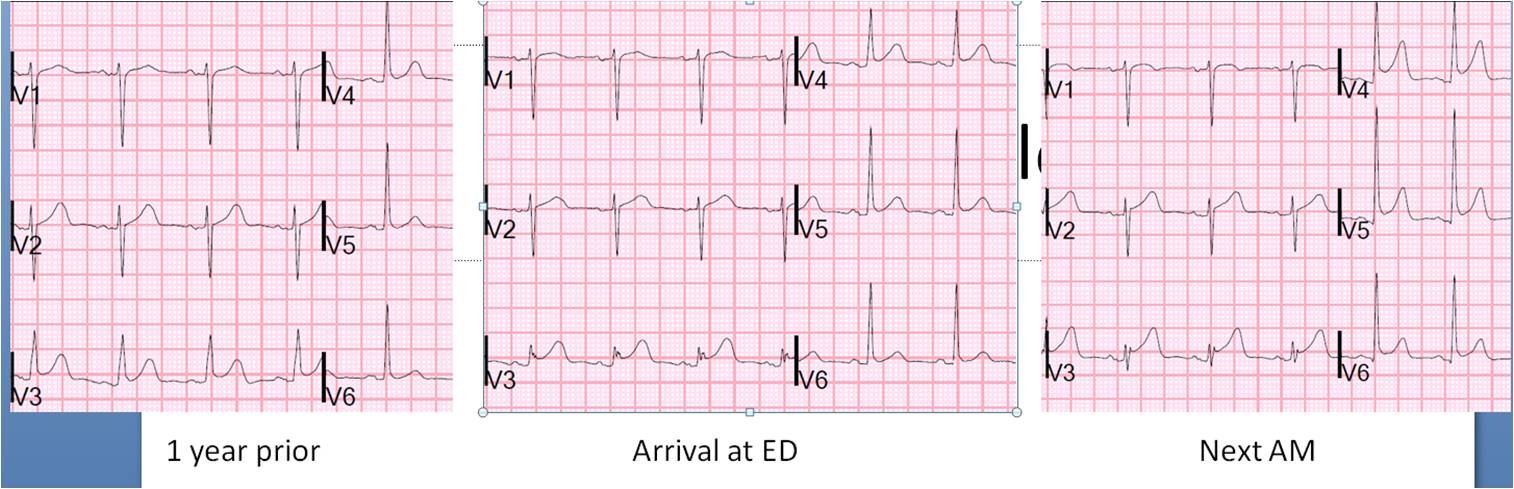
This was recorded the next AM, after the patient had ruled out with serial troponins:
Here are all 3 side by side:
Case 2.
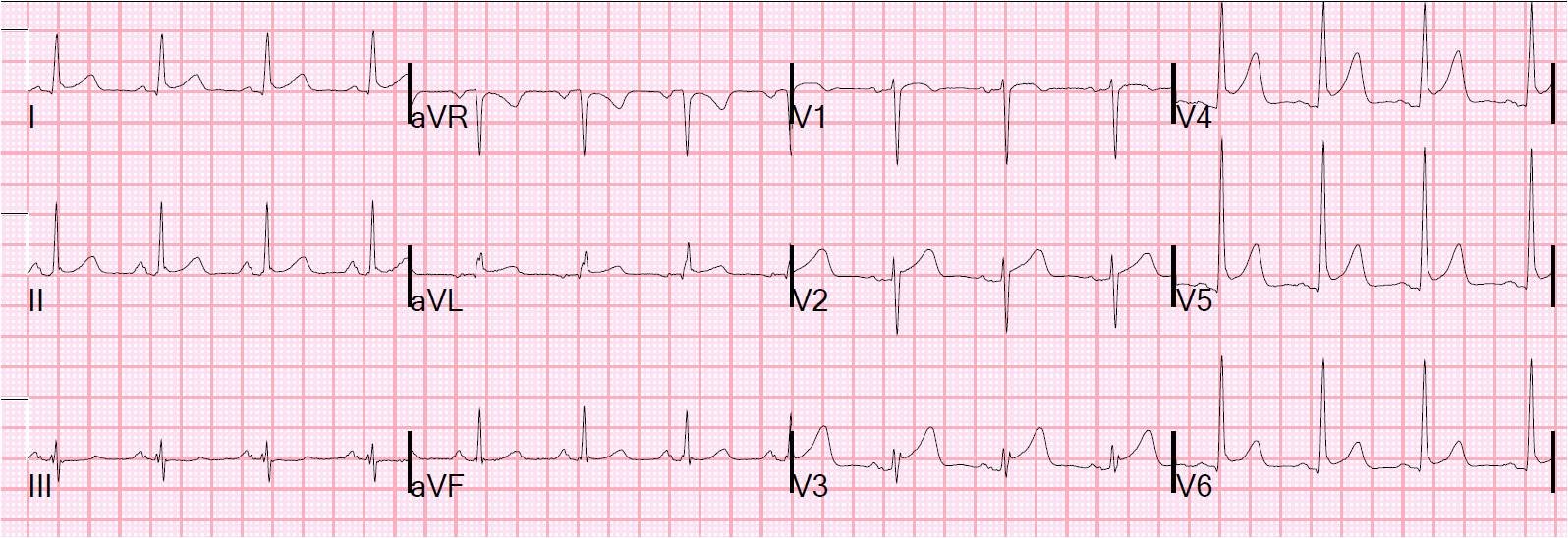
A Hennepin residency graduate called me to ask about an ECG. I happened to be in the ED so I asked her to fax it. She was worried about diffuse ST elevation and whether there was MI or pericarditis.
 |
| There is 4 mm of STE at 60 ms after the J-point (2.5 mm at the J-point) in V2, so it looks scary. There is 1 mm STE in 2 consecutive of inferior and lateral leads. So it meets “criteria” for fibrinolytic therapy in every coronary distribution. But the computerized QTc is 370 ms, the STE at 60 ms after the J-point in V3 is only 2mm, and the R-wave in V4 is 19 mm. Equation value is 21.08, so this is unlikely to be an anterior STEMI. Is it lateral or inferior STEMI? The pronounced J-waves make early repol in inferior or lateral walls much more likely than STEMI. The absence of reciprocal ST depression in aVL makess inferior MI extremely unlikely. |
As for pericarditis: the ratio of ST elevation to T-wave in V6 is less than 25 percent, so pericarditis is unlikely. Furthermore, there is no significant PR segment depression.
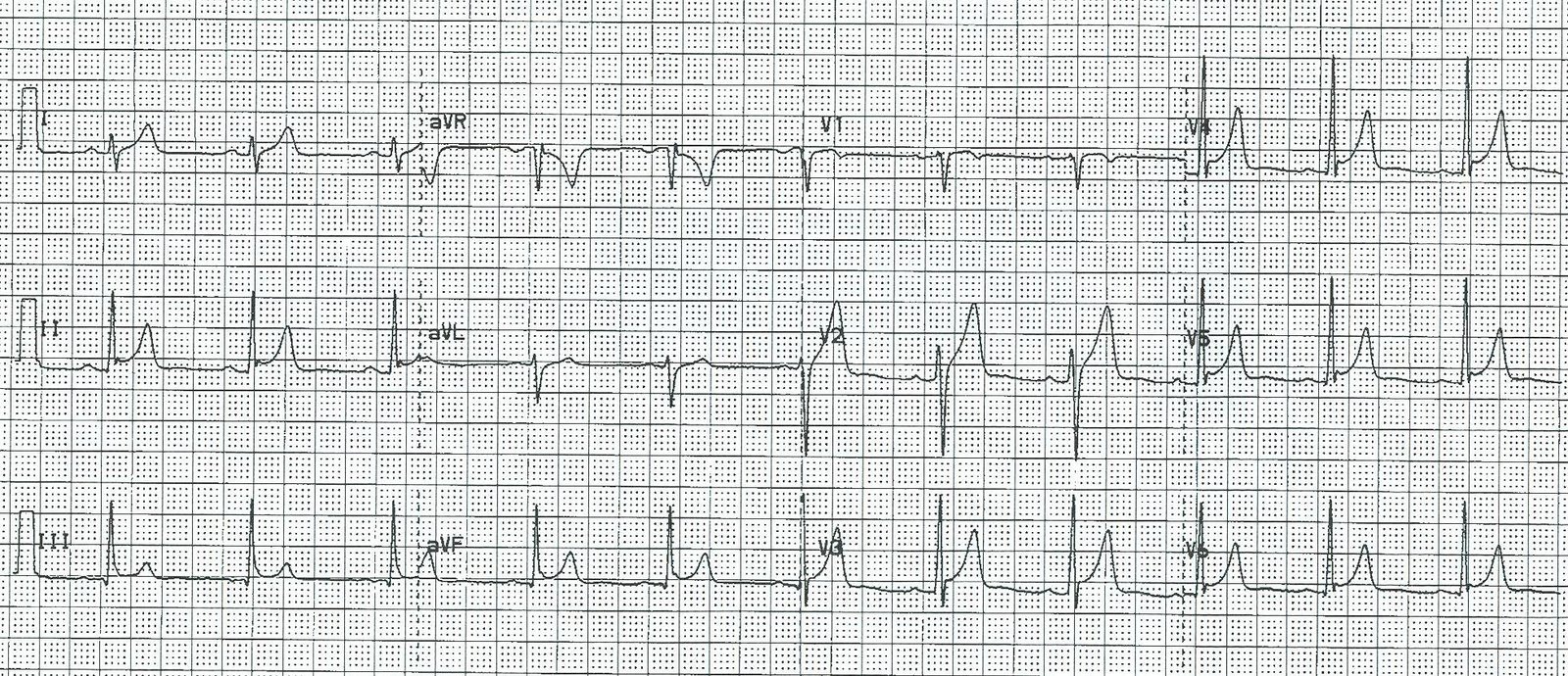
Case 3. A 19 yo with stab wound to the chest. After viewing the ECG, there was concern for LAD laceration.
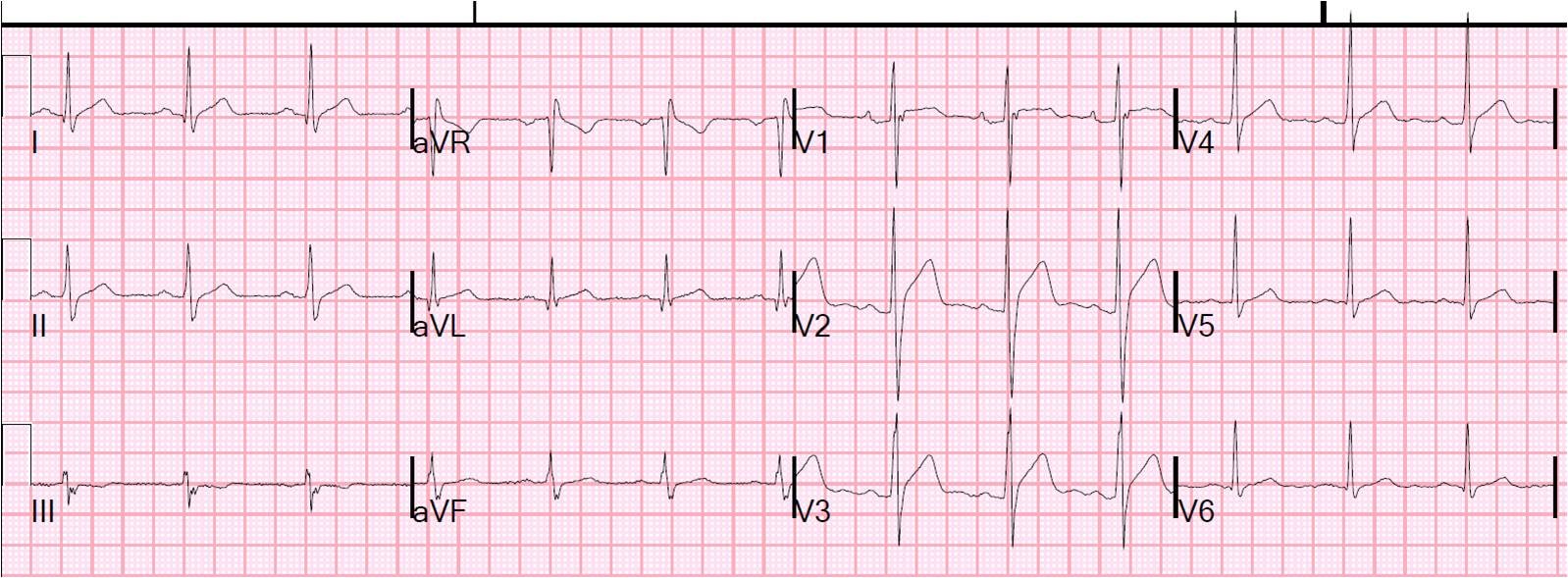 |
| Again, there is scary ST elevation. In fact, the ST segments in V2 and V3 are straight, not concave. In my study, I excluded ECGs with non-concave (straight or convex) ST segments because they are so specific for STEMI. Nevertheless, if you apply the equation, the value is only 20.52. The patient ruled out. The heart was not affected by the stab wound. |