This is a case I had about a decade ago.
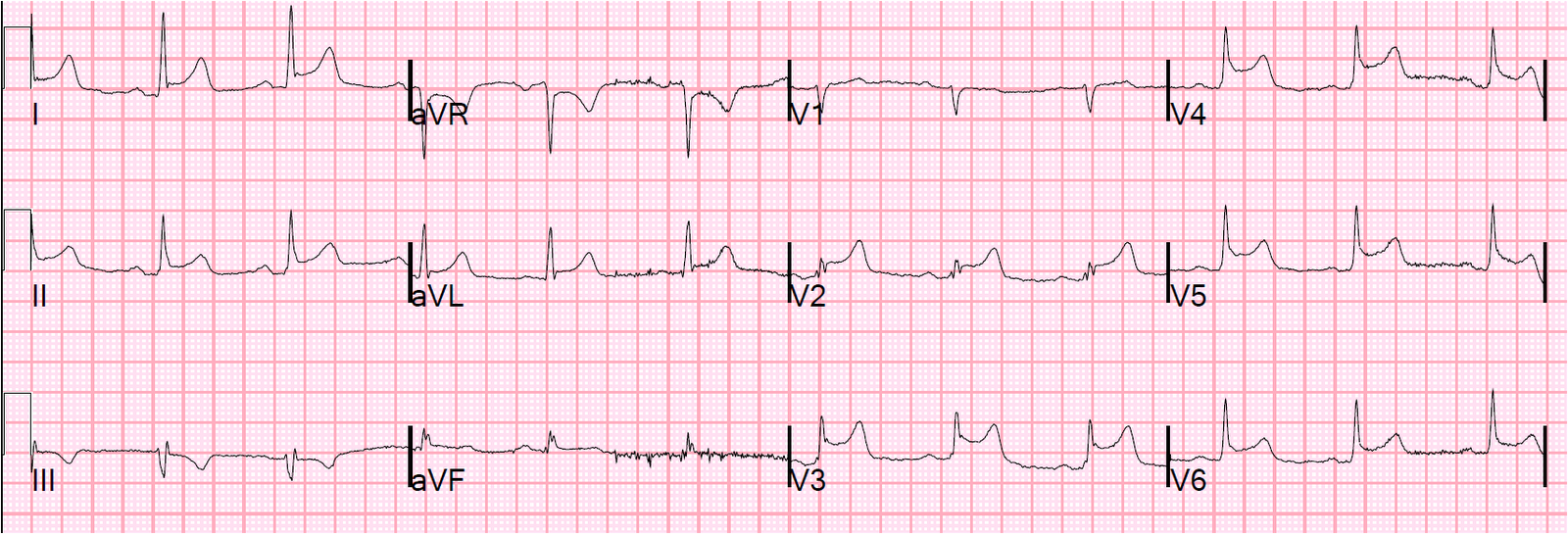
This is a 51 year old who was playing cards with his friends when he started to have left hand numbness. They were worried he was having a stroke and so called 911. The medics had just learned to do ECGs, and so recorded one. Here it is, at 1915:
 |
|
|
I activated the cath lab at 1929 based on this ECG.
Then, I questioned the patient at length and his only symptom was subjective left hand paresthesias. He had no pain, discomfort, or tightness of any kind, no weakness, and no SOB. So I had a hard time believing the ECG. I thought perhaps it was recorded with lead misplacement.
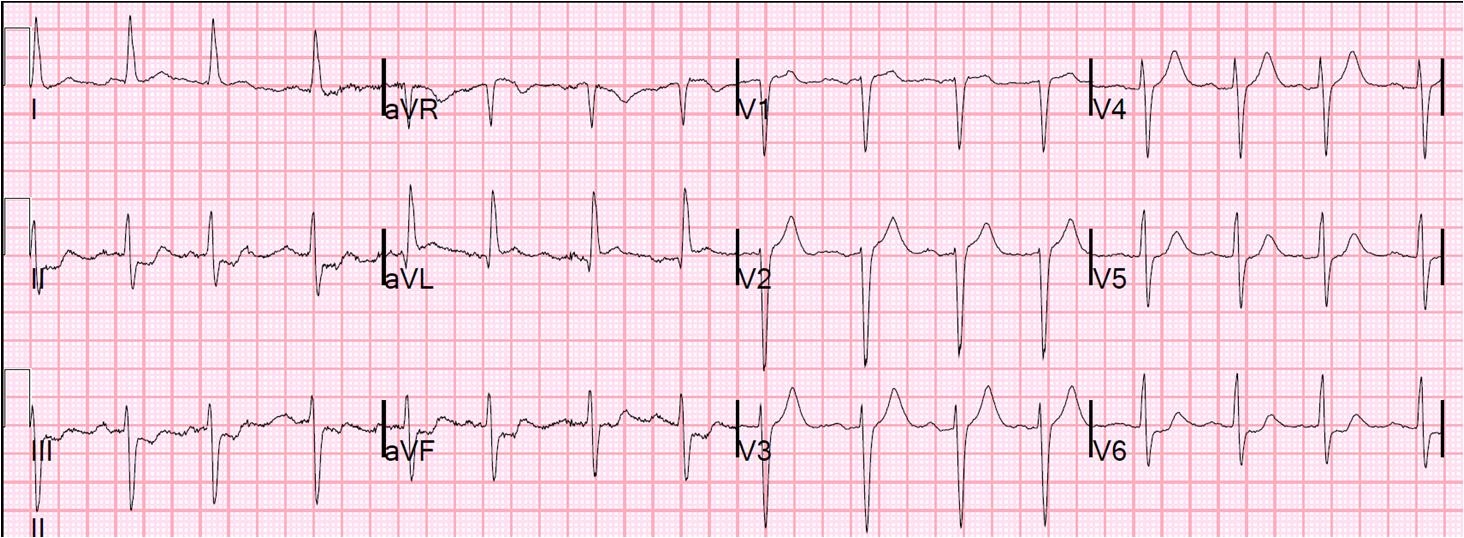
So I did the first ED ECG at 1931:
 |
|
|
With no more overt STEMI, and (through bad thinking and “Nah, couldn’t be…..”) I thought that there must have been some mistake in recording the first ECG. At worst, if it was a STEMI, I thought that it is reperfused. I cancelled the cath lab activation for the team that would have to come in from home.
(Today I would have unequivocally interpreted leads V2 and V3 as LAD occlusion).
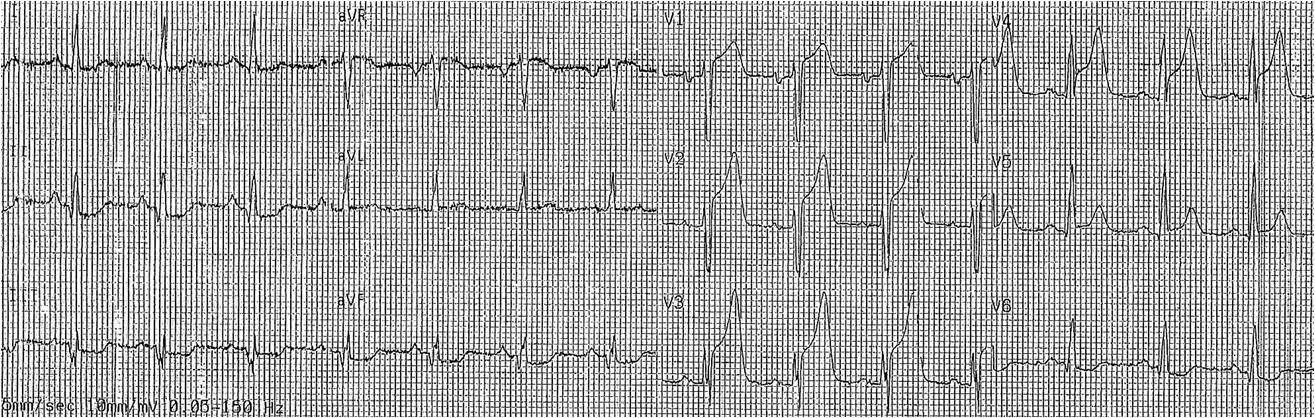
At 1942, the patient started becoming hypotensive, so I recorded another ECG at 1946:
 |
|
|
I activated the cath lab again at 1946, so that I had caused a 17 minute delay by cancelling.
He went to the cath lab, had an LAD occlusion, then died just before it could be opened.
I learned 2 major lessons from this:
1. STEMI, even if it spontaneously resolves, is very high risk and must go to the cath lab.
2. A clearly diagnostic ECG is diagnostic even if it does not match the symptoms.
(One cannot make the same conclusion about ECGs that are only highly suspicious – these are more likely to be false positives in the context of atypical symptoms.)