This 56 year old male presented with atypical chest pain and left arm numbness off and on for one week, worse on the day of presentation:
 |
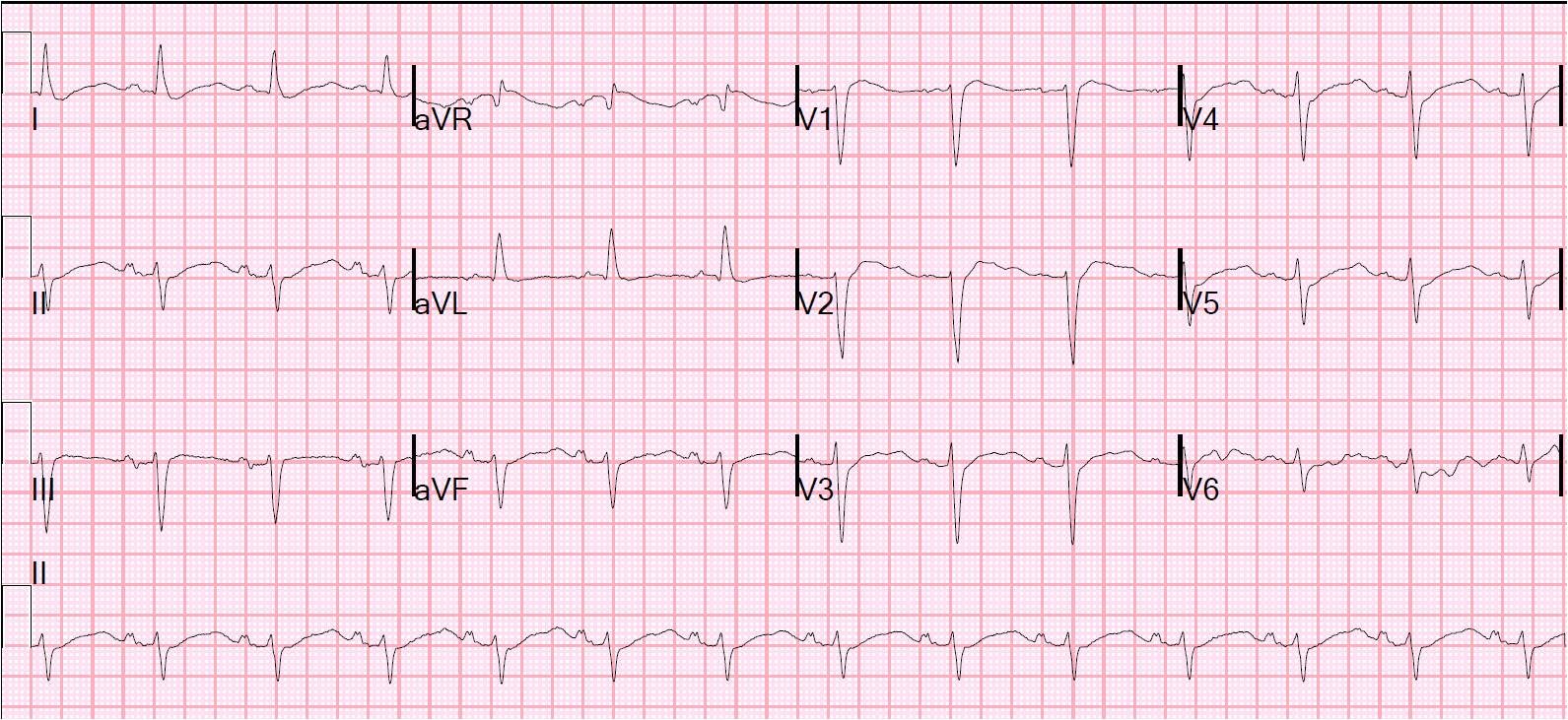
| There is saddleback type ST elevation in leads V2 and V3, and diffuse T-wave inversion. But there is also very high voltage especially in V4 (35mm, sorry it is cut off) and V5 (27 mm). The QTc was 426 ms. |
Answer is below:
This ECG was shown to me by a colleague, and I immediately said: “You thought it was a STEMI, but it is not.” He had, in fact, activated the cath lab, and the coronaries were clean and the patient ruled out.
Saddleback ST elevation, in my experience, is rarely due to STEMI. I will not say it is never due to STEMI because I know of no research on this topic. It is usually a form of early repolarization that also usually meets criteria for type II or III Brugada pattern (see this post). I will post more on this topic later. In this case, it may be related to the LVH or be simultaneous early repolarization and LVH. The diffuse (both inferior and precordial) T-wave inversion is somewhat atypical of LVH.
Echocardiography confirmed marked concentric LVH.
In this case, you might want to try applying the early repol/anterior STEMI equation rule posted on the sidebar. However, it is not validated in the presence of LVH). You would get a value of 16.11, which is very low and argues strongly against LAD occlusion.