A middle-aged male with a history of 2-vessel coronary bypass called 911 because of the relatively sudden onset of severe SOB. He had had more mild SOB for the past 2 days. The medics found him in respiratory distress with coarse breath sounds, a BP of 196/132, oxygen saturations of 90%, and a pulse of 130. They put him on CPAP for respiratory support. He denied chest pain.
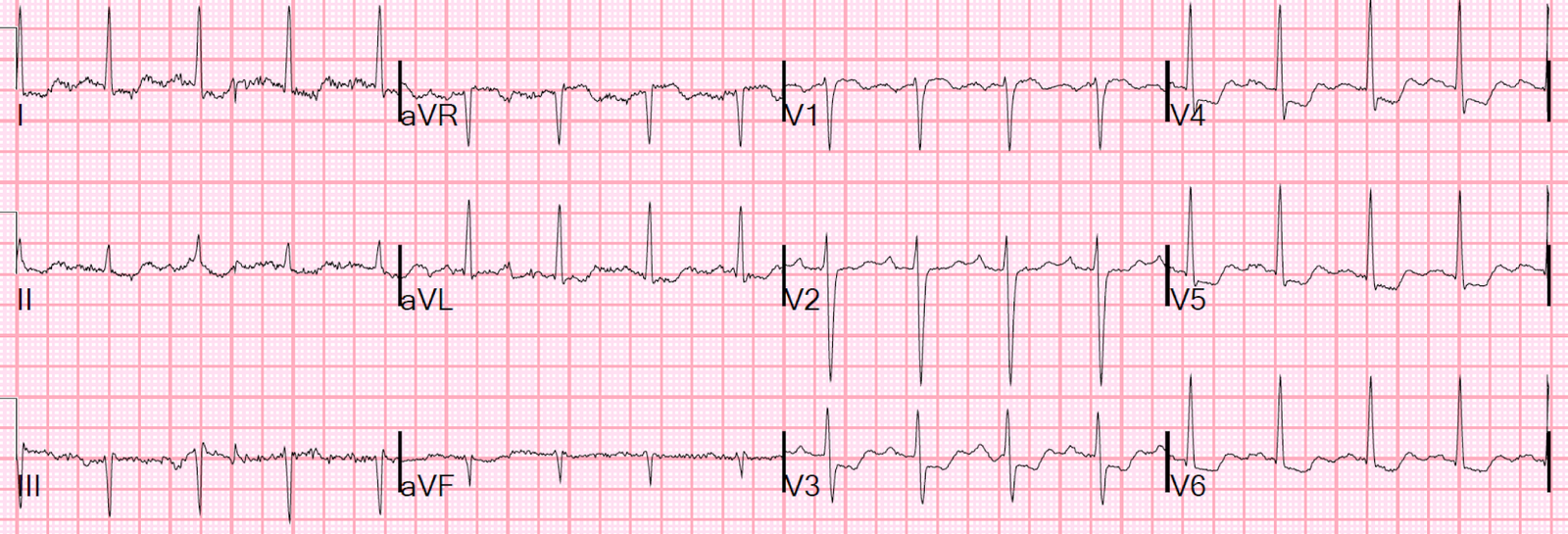
Here is his prehospital ECG:
 |
| There is diffuse ST depression, with ST elevation in lead aVR |
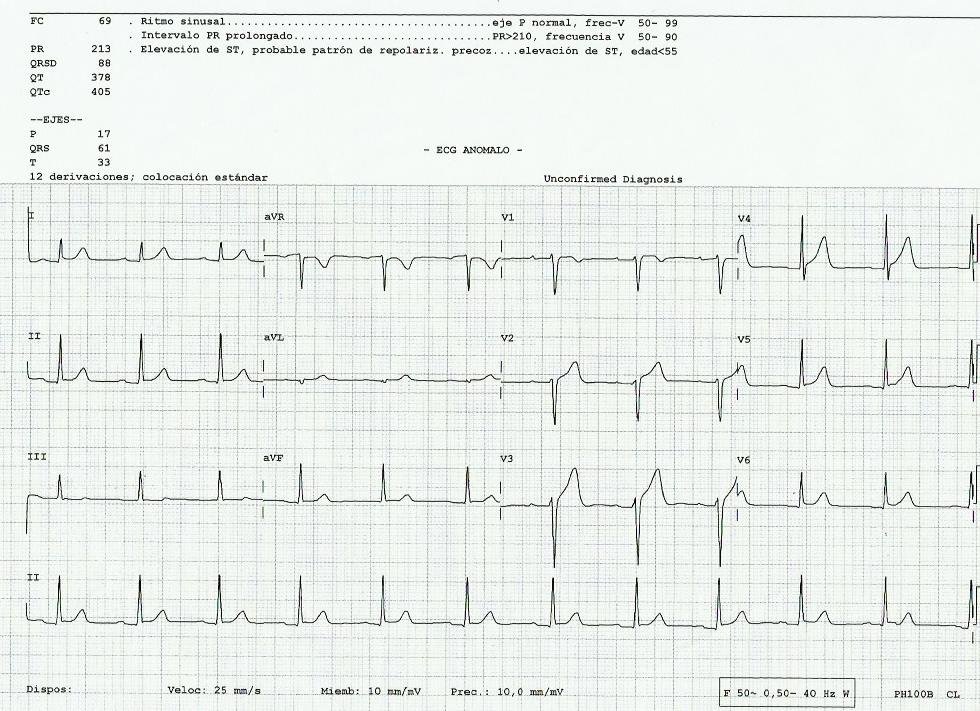
The patient arrived in the ED and was put on Noninvasive ventilation (BiPAP). Blood Pressure was 200/110. A nitroglycerin drip was started and this ECG was recorded:
 |
| Same as prehospital
The ischemia could be due to supply/demand ischemia from hypoxia, tachycardia, and hypertension, or it could have been initiated by ACS. The ECG cannot differentiate. If ACS, it could be diffuse subendocardial ischemia, or posterior STEMI. Does that matter? |
Bedside echo showed diffuse B-lines of pulmonary edema.
The plan was to completely control the blood pressure and re-assess for ischemia.
BP was controlled to 120/70 with very high dose Nitro, and the patient’s respiratory distress was improved, and another ECG was recorded:
 |
| Continued ST depression |
Now we have controlled the excessive demand but the ischemia persists: the BP is not elevated, the heart rate is only mildly elevated, there is no more hypoxia, the hemoglobin returned normal, and there is no evidence of valvular dysfunction (at least no murmur).
Thus, ACS is very likely the initiating factor. So we have ACS with both refractory symptoms and pulmonary edema, both of which are indications for cath lab activation.
ST depression in the precordial leads can be either posterior STEMI or diffuse subendocardial ischemia. Does this matter? No! This is ACS that needs the cath lab now because it is refractory to medical management.
There are those who think this ECG pattern in ACS is due to left main occlusion. This is not accurate. See this exhaustive post on the topic.
The cath lab was activated.
Normally, a P2Y12 inhibitor (clopidogrel, ticagrelor) would be given, but in this case with STE in aVR and diffuse ST depression, there is high potential for left main insufficiency or severe 3 vessel disease. Thus, there was approximately a 50% likelihood that the patient would need CABG (surgical bypass), although this probability is less in a patient with previous bypass. Clopidogrel or even ticagrelor would increase the risk of severe bleeding at surgery.
Thus, eptifibatide was given instead of ticagrelor. Eptifibatide can be turned off.
The patient could not lie flat and so was intubated.
The patient went to the cath lab and had a 100% mid circumflex occlusion that was opened. Since bypass would not be needed, ticagrelor was initiated.
The outcome was good except for some bleeding complications, during which time his P2Y12 inhibitor (ticagrelor) needed to be held.
The echocardiogram confirmed a posterior wall motion abnormality. The troponin I peaked at 20 ng/mL.
Epilogue
The patient returned a few weeks later with the identical presentation: respiratory failure, pulmonary edema, and severe hypertension. His ECG is shown here:
 |
| There is diffuse ST depression and ST elevation in aVR, although not as profound as the first time |
After treatment with BiPAP and IV Nitroglycerin, his symptoms greatly improved and this ECG was recorded:
 |
| The supply/demand issues are gone and the ST depression is resolved. |
Because of the recent stent and the time off of clopidogrel, an angiogram was done and showed no in-stent thrombosis (no new ACS). The troponin peaked at 1.5 ng/mL and there was no new wall motion abnormality.
This ST Depression was due entirely to supply/demand mismatch, not due to ACS. The second presentation was purely a type II MI.
Learning Points:
1. In the setting of ischemia, before diagnosing ACS, manage the oxygen supply and demand issues first. Use supportive care. Then re-assess. If ischemia persists, then it is ACS.
2. If ACS and symptoms are refractory, it does not matter whether it is a posterior STEMI or diffuse subendocardial ischemia. Emergent angiogram and PCI if indicated should be undertaken.