There are many publications stating that ST elevation in lead aVR, with diffuse ST depression elsewhere, is due to left main (LM) occlusion. This is even stated in the lastest 2013 ACC/AHA STEMI guidelines (O’Gara PT et al. JACC 61(4):e83; January 29, 2013). However, the guidelines use as evidence an article by Jong et al. (Int Ht J 2006; 47(1):13-20). That article misleadingly defines “occlusion” as any stenosis greater than 50%, when it should rather be defined as 100%, or nearly so. All of the articles that claim ST elevation in aVR is a sign of LM occlusion confuse LM occlusion with LM insufficiency. In reality, ischemic ST elevation in aVR occurs in two broad categories: 1) in patients with recognized STEMI (due to coronary occlusion, usually of the LAD) and is associated with higher mortality than in patients without STE in aVR and 2) in patients without ischemic ST elevation, in which case there is always diffuse ST depression of subendocardial ischemia (which can be due to supply-demand mismatch or due to ACS). If due to ACS, this STE in aVR is associated not only with acute LM insufficiency, but alternatively with 3 vessel disease, or with LAD insufficiency.
Knotts et al. found that only 23% of patients with the aVR STE pattern had any LM disease (fewer if defined as ≥ 50% stenosis). Only 28% of patients had ACS of any vessel, and, of those patients, the LM was the culprit in just 49% (14% of all cases). It was a baseline finding in 62% of patients, usually due to LVH. Reference: Knotts RJ, Wilson JM, Kim E, Huang HD, Birnbaum Y. Diffuse ST depression with ST elevation in aVR: Is this pattern specific for global ischemia due to left main coronary artery
disease? J Electrocardiol 2013;46:240-8.
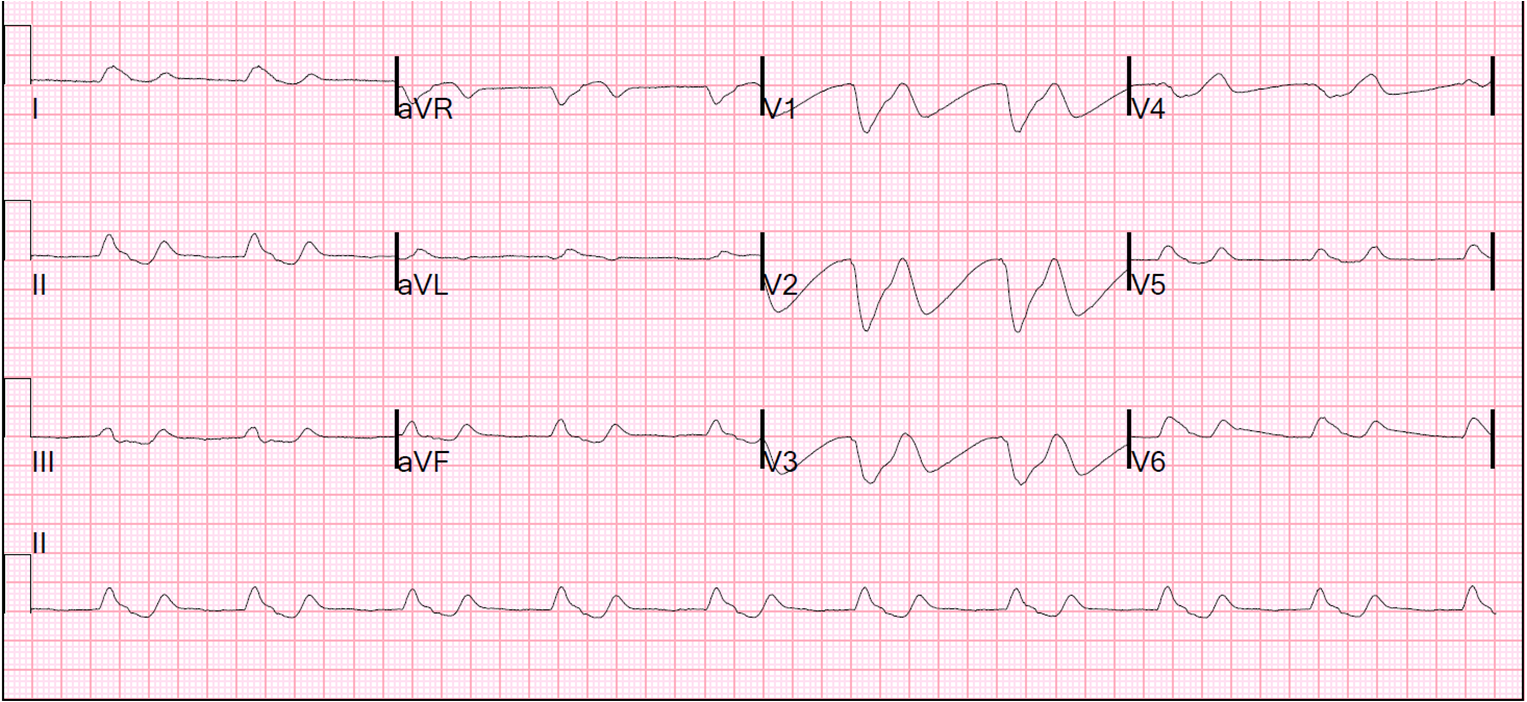
See this ECG in a patient with acute chest pain:
 |
|
There is diffuse ST depression, with ST elevation in aVR. This is diffuse subendocardial ischemia. The Here is the angiogram: |
 |
|
There is a very tight stenosis that limits the blood flow, but there is clearly flow in all the arteries supplied by the left |
The subendocardium is more susceptible to ischemia than the epicardium due to its proximity to the high pressure LV chamber and also because of its distance from the epicardial coronary arteries (the arteries that penetrate to the endocardium must travel a longer distance and go through the high pressure myocardium to the high pressure endocardium).
Of course, this is a very dangerous situation: the myocardium is ischemic, and if it is due to thrombus (due to ACS), then the thrombus can and often does propagate to occlude the entire artery and then result in STEMI.
Must you activate the cath lab in this situation?
Rokos et al. call this a “STEMI-equivalent” and suggest that the
patient should go immediately to the cath lab (Rokos IC et al. Catheterization and Cardiovasc Interventions 79:1092-1098; 2012). However, in the data they present in this paper, there were 11 patients with true left main occlusion; 5 of them had ST elevation in lead aVR. But if one must read the fine print to realize that all 11 patients with the left main as the culprit vessel were enrolled in the study based upon the standard STEMI criteria on index ECG: 8 anterior, 1 inferior, 1 LBBB, and 1 without an ECG submitted to the core laboratory. In other words, these were STEMI that were already diagnosed as STEMI who also had ST elevation in lead aVR; one did not need lead aVR in order to make the diagnosis of STEMI.
The conundrum arises when there is STE in aVR and ST depression in many other leads, and thus it is not a classic STEMI. Is this situation a STEMI-equivalent?
As explained above, such ST depression with STE in aVR signifies diffuse subendocardial ischemia and is just as common in Non-ACS etiologies of ischemia (supply-demand mismatch) as in ACS etiologies. This is common in patients with GI bleed, sepsis, respiratory failure, severe anemia, tachydysrhythmias, severe hypertension, shock, and more.
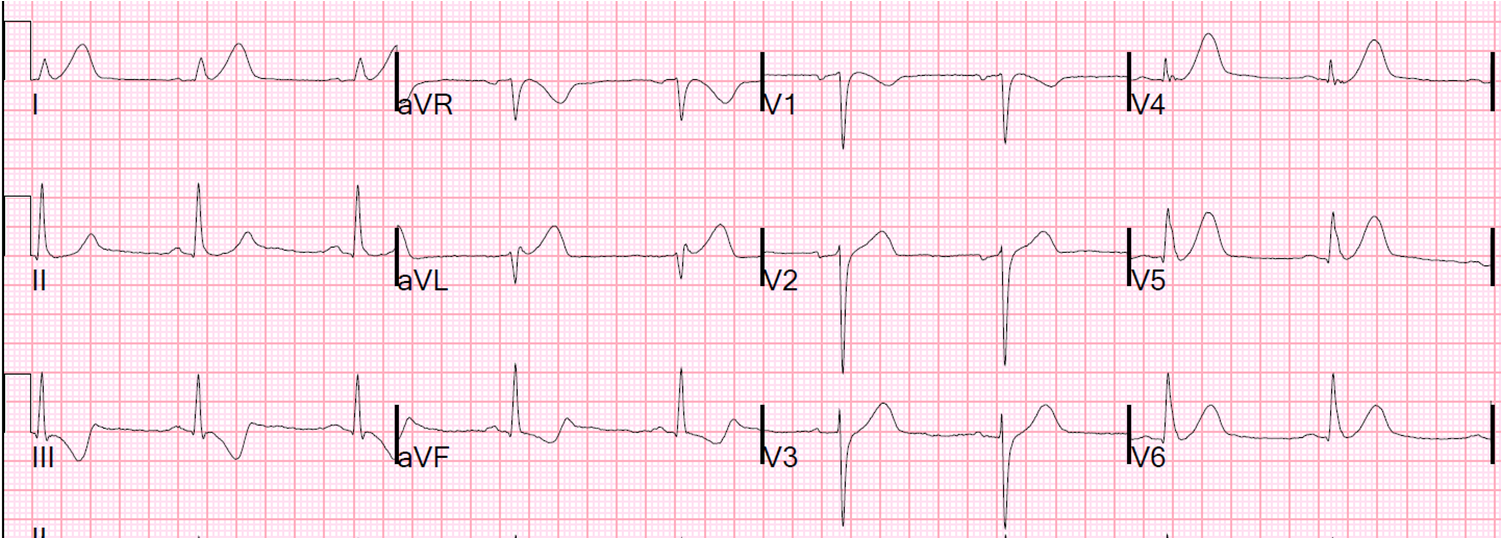
For instance, see this case of carbon monoxide poisoning, with a CO level of 28%:
 |
| Diffuse ST depression with STE in aVR. It all resolved after hyperbaric therapy. There was no ACS. |
Cath lab activation should only be done for ACS. For non-ACS etiologies of
diffuse ST depression, treat the underlying illness!
Of course, it is not always easy to determine which came first, ACS or other
underlying illness:
1)
Did ACS initiate the ischemia, which then resulted in cardiogenic
shock, which then resulted in pulmonary edema with hypoxia, respiratory
failure, and tachycardia?
2)
Or was the inciting factor bleeding, hypoxia, or severe hypertension with
pulmonary edema and subsequent ischemia?
This
requires careful patient evaluation of volume status, laboratory values, presence of pulmonary edema and of course much more. One must evaluate the patient, with help
from the ECG.
The patient who has ST elevation in lead aVR that is not due to ACS will have appropriate treatment delayed and will undergo harm with cath lab activation.
Furthermore, as stated above, even if STE in aVR with diffuse ST depression is indeed due to ACS, it implies open arteries, not occluded ones. There are institutions in which
cath lab activation is a major use of resources, and if cath lab activation at night is not absolutely necessary, then it may be okay to avoid it. When there is diffuse subendocardial ischemia (which may or may not be left main insufficiency, but could also be LAD insufficiency, or 3 vessel insufficiency), it is reasonable to treat medically with nitroglycerine, aspirin, antithrombotics, and dual or triple antiplatelet therapy, and to re-assess.
Often, the thrombus will cool off and the chest pain and ECG findings will resolve (both must resolve!). If the symptoms resolve and the ST depression greatly improves, then the patient can wait for the morning to go to the cath lab as long as there is very close monitoring, preferably with continues 12-lead ST segment monitoring. Ischemia due to ACS that is refractory to medical therapy (persistent symptoms or persistent ECG findings) requiresemergent cath.
Left Main Occlusion
The majority of 100% left main occlusions do not make it alive
to the ED, or arrive in arrest. At cath, only 0.19% – 1.3% of STEMI
patients have LMCA occlusion (or 0.42% – 3% of anterior STEMI).
Below is the ECG of a patient who collapsed in v fib, underwent prolonged
resuscitation and had return of spontaneous circulation, but was in cardiogenic shock:
Prehospital ECG:
 |
|
Both the rhythm and QRST are difficult to |
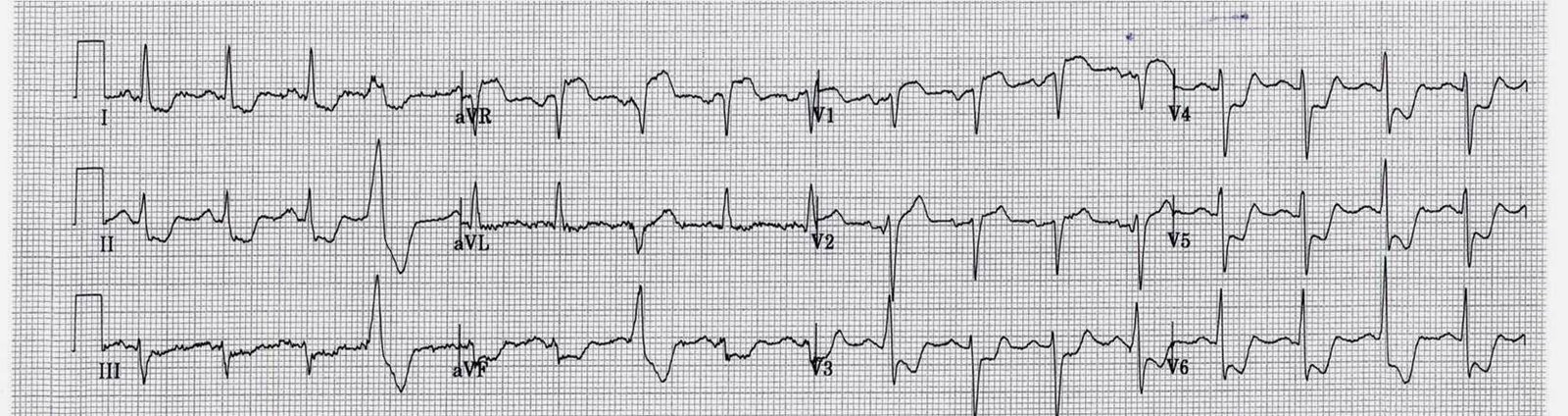
ED ECG:
 |
| See explanation below the annotated version |
Here is an annotated version:
 |
| I have used lead II across the bottom to find the end of the QRS, then drawn a ling upward to find the end of the QRS in all other leads. This helps to find the beginning of the ST segment. |
This ECG is typical of a patient with left main OCCLUSION. In fact, it was not exactly LM occlusion, but rather simultaneous LAD and Circumflex occlusion, which is in effect the same problem.
–The rhythm again is difficult. There appear to be non-conducted P-waves. It may be supraventricular or nodal, or it could be idioventricular.
–There is a wide complex. If supraventricular, this is RBBB + LAFB (often seen in massive MI). If idioventricular, then it is originating near the left posterior fascicle, which then mimics RBBB + LAFB.
—In any case, there is ST elevation in I and aVL (high lateral MI) with reciprocal STD in inferior leads. There is also ST elevation in V2 and V4-V6.
Left Main occlusion results in an ECG with overlapping syndromes of proximal LAD occlusion (STE in V1-V6, I, aVL) and circumflex occlusion (lateral STE and posterior STEMI, which has ST depression in V1-V4, which may diminish the ST elevation of the anterior STEMI.
How does Acute Total Left Main Coronary occlusion present on the ECG?
Below is the clearest discussion of Lead aVR in ACS that you will find.
Note it is divided into a 1) general discussion (short) 2) aVR in STEMI and 3) aVR in Non STE-ACS
The following article on aVR in ACS is taken from an article I wrote in 2013. Full text is available here. This excerpt is reprinted from Smith SW. Updates on the Electrocardiogram in Acute Coronary Syndromes. Current Emergency and Hospital Medicine Reports 2013; 1(1): 43-52.
1. Lead
aVR in Acute Coronary Syndromes.
It is important to note that when I use the term “left main disease” I do not refer to occlusion but to insufficiency; that is, enough obstruction to cause ischemia, but not fully occluded.
There is a body of literature in the past decade on the significance of ST-segment elevation in lead aVR in ACS, and especially for its significance for diagnosis of left main coronary artery (LMCA) obstruction and 3-vessel disease.63-68 The literature is confusing for a few reasons. First, studies do not always clearly distinguish patients with and without STEMI. Second, LMCA “obstruction” is rarely defined, leaving it ambiguous as to whether the obstruction is 1) complete, 2) incomplete (subtotal), 3) complete but with good collateral circulation or 4) intermittent. Third, the studies were nearly all small with a retrospectively identified group with LMCA ACS. Fourth, findings may be influence by individual anatomy, ischemic preconditioning, and
the timing of ECG recording. Since patients with LMCA occlusion do not often survive to the cath lab, the pretest probability for any positive ECG findings is low, and any reported sensitivities and specificities may distort the clinician’s assessment of the actual presence of disease.
Lead
aVR in STEMI
Lead aVR in STEMI
is touted as important for recognizing LMCA occlusion.68 Since patients with STEMI are already identified as a group which needs immediate reperfusion therapy, the primary importance of recognizing LMCA involvement in STEMI is 1) to recognize the increased mortality associated with this finding and 2) in the potential to avoid thienopyridine (e.g., clopidogrel) administration in such patients who are likely to need CABG and may suffer from excessive bleeding if they do receive a thienopyridine.
Only 0.19% – 1.3% of STEMI patients have LMCA occlusion, or 0.42% – 3% of anterior STEMI,69, 70 partly because patients with occlusion do not frequently survive to the cath lab. Mortality is 50%, and over 70% present in cardiogenic shock, such that the diagnosis of severe ACS and need for cath lab activation is usually apparent from the clinical presentation, rather than the ECG. In contrast, approximately 10% of
patients with anterior STEMI have STE of at least 1 mm in aVR (as measured at
60 ms after the J-point),66 and 25% have at least 0.5 mm STE in aVR (as measured at 60 ms after the J-point, relative to the TP segment).63 STE or STD of 1 mm or more in
anterior STEMI portended a worse prognosis (compared to no STE or STD), even
after correcting for STE or STD elsewhere on the ECG, but only ST depression in
aVR (“reciprocal to injury in the area of lead V7”) remained significant when
corrected for all other ECG and clinical factors.66
STE in aVR of at least 0.5 mm in anterior STEMI predicts septal AMI (occlusion of the LAD proximal to the first septal perforator) with a PPV and NPV of 70% and 80%63 better than STE in V1, which at a cutoff of > 2.5 mm had 12% sensitivity and 100% specificity, with PPV and NPV of 100% and 39%.71 Kotoku et al.64 similarly found that STE in aVR correlated with proximal (vs. distal) LAD occlusion and was negatively
correlated with a long (vs. short), or wraparound, LAD that affected the inferior wall. This is intuitive, as a proximal occlusion would lead to basal wall STEMI (see below), and distal occlusion of a wraparound (long, “type III”) LAD would lead to inferior STE
which would reciprocally attenuate the STE in aVR, or lead to STD in aVR. To be complete, Wong also found that STE in aVR in inferior STEMI conferred worse
outcomes.66
The study by Yamajiet al. is cited as evidence that STE in aVR > STE in V1 is 81% sensitive and 80% specific for identifying the LMCA as the culprit.72 [Incidentally, this study has been cited among the general ACS literature;68 however, it applies to STEMI only, as methods required TIMI 0-1 flow.] If its conclusions are accurate, and one considers that 0.4%-3% of LMCA occlusions make it to the cath lab alive, then the positive predictive value (PPV) of STE in aVR greater than STE in V1 is only 1.6%-11%, rendering this finding useless. Furthermore, in the study by Kurisu et al. of consecutive STEMI, written as a letter, 25 (about 3% of those with anterior STE) had LMCA occlusion; they compared ECG measurements of the 25 LMCA occlusions to only 30 each of consecutive LAD, RCA, and circumflex occlusions and found sensitivity and specificity for LMCA, vs. LAD, of STE in aVR greater than STE in V1 of 40% and 93%, resulting in a PPV of only 15%.70
A suggested explanation for STE in aVR greater than V1 in LMCA STEMI (due to occlusion) is that aVR overlies the injured basal septum. The STE registered in V1, and presumably also other right precordial leads V2-V4, is partly attenuated by the reciprocal ST depression of the posterior wall STEMI that is due to obstruction of flow in the circumflex artery. The most likely explanation for STE in both aVL and aVR is similar: in addition to anterior and basal septal STEMI, there is high lateral STEMI from absence of circumflex flow, such that the ST vector is superior (a “superior” STEMI), as well as anterior.65
Lead
aVR in Non-STE-ACS
Lead aVR has been ignored in the past because it is 180° opposite from an imaginary lead between leads I and II, and therefore would provide no independent data. More recent claims that ST elevation in aVR is independent of ST depression in these opposing leads have not been substantiated for Non-STEMI, though this appears to be true for STEMI (see above). Nevertheless, it is convenient to use one lead with ST elevation (aVR) as a substitute for many others with ST depression, such that, in Non-STE-ACS, the degree of ST elevation in aVR correlates with the number of leads with ST depression, the depth of the ST depression, and the sum of ST depressions.67, 73-76
In all studies, measurements of the ST segment are at 80 ms after the J-point for ST depression and 20 ms after the J-point for ST elevation, both relative to the TP segment.
To very briefly summarize the literature, diffuse ST depression has a good PPV and NPV for 3-vessel and left main disease (not occlusion!).73, 77 The degree of STE in aVR, though not independent of ST depression, has strong association with outcome independent of clinical factors such as Killip class and blood pressure.74, 76 Barrabes et al. studied 775 Non-STEMIs and found that, compared to no STE in aVR, STE of 0.5 to 1.0 mm had odds ratio (OR) for death of 4.2 (1.5 – 12.2), and STE of ≥ 1.0 mm had OR of 6.6 (2.5 – 17.6).74 There were 475 who underwent angiography; of those with ≥ 1 mm of STE in aVR (n=92), 48% had 3 vessel disease and 18% had LMCA disease, compared to 21% and 4% for those with less than 1 mm STE in aVR.74 Kosuge et al.75 (2005) studied 310 patients with ACS without STE. They found that STE in
aVR of ≥ 0.5 mm was the strongest predictor of LMCA or 3-vessel disease, with an
OR of 19.7, and it identified LMCA or 3-vessel disease with 78% sensitivity and
86% specificity, and a PPV and NPV of 57% and 95%. Finally, Szymanski et al. in 2008 found mortality correlated with the degree of STE in lead aVR, independent of TIMI score, and was highly associated with ST depression in multiple locations.
In 2011, Kosuge et al.67 studied 572 patients with Non-STE-ACS; among the 196 with a positive troponin T on admission, the sensitivity and specificity of STE ≥ 1.0 mm in aVR for LMCA or 3-vessel disease was 80% and 93%, with a PPV of 56% and an NPV of 98%, and accuracy of 92%. OR of degree of STE in aVR for severe 3-vessel or LMCA disease among all patients was 29 (9.5 – 50). CABG was undertaken in 46%
of those with severe 3-vessel or LMCA disease vs. 2% of those without. The authors suggest withholding clopidogrel in patients with Non-STEMI and STE in aVR of at least 1 mm.
Summary
of lead aVR in ACS:
Thus, STE in aVR in Non-STEMI, though not independent of ST depression
elsewhere, is a good approximation of the sum of STD and is a very useful
predictor of poor outcomes and of need for CABG, independent of other clinical
data. In Non STE-ACS, STE in aVR is reciprocal to diffuse ST depression, opposite (reciprocal) to a negative ST vector towards I, II, and V5, and is a result of subendocardial ischemia.
On the other hand, the STE in aVR in STEMI, usually anterior STEMI, is more likely a result of transmural injury (STEMI of the basal septum). In this latter case the STE in aVR is not reciprocal to any ST depression, but directly indicative of injury.
Finally, the most relevant practical applications are:
1) In Non-STEMI, if there is STE in aVR ≥ 1.0 mm, it may be prudent to withhold clopidogrel
2) In both STEMI and Non-STEMI, the degree of STE in aVR correlates with
worse disease and worse outcomes, independent of the clinical presentation; these patients must be treated aggressively with early angiography and revascularization.
References
STEMI -equivalents:
1. Jong, GP et al. Reciprocal Changes in 12-Lead Electrocardiography Can Predict Left Main Coronary Artery Lesion in Patients With Acute Myocardial Infarction. International Heart Journal 47:13-20; 2006.
2. Rokos IC et al. Correlation Between Index Electrocardiographic Patterns and Pre-Intervention Angiographic Findings: Insights From the HORIZONS-AMI Trial. Catheterization and Cardiovascular Interventions 79:1092-1098; 2012.
3. Rokos IC. French WJ.
Mattu A et al. Appropriate Cardiac Cath Lab activation: Optimizing electrocardiogram interpretation and clinical decision making for acute ST-elevation myocardial infarction. Am Heart J 2010;160:995-1003.e8
63. Aygul N, Ozdemir K, Tokac M, et al. Value of lead aVR in predicting acute occlusion of proximal left anterior descending coronary artery and in-hospital outcome in ST-elevation myocardial infarction: an electrocardiographic predictor of poor prognosis. J Electrocardiol 2008;41(4):335-41.
64. Kotoku M, Tamura A, Abe Y, Kadota J. Determinants of ST-segment level in lead aVR in anterior wall acute myocardial infarction with ST-segment elevation. J Electrocardiol 2009;42(2):112-7.
65. Nikus KC, Eskola MJ. Electrocardiogram patterns in acute left main coronary artery occlusion. J Electrocardiol 2008;41(6):626-9.
66. Wong CK, Gao W, Stewart RA, French JK, Aylward PE, White HD. The prognostic meaning of the full spectrum of aVR ST-segment changes in acute myocardial infarction. Eur Heart J 2012;33(3):384-92.
67. Kosuge M, Ebina T, Hibi K, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol 2011;107(4):495-500.
68. Lead aVR: Importance of the “Forgotten 12th Lead” in Patients With ACS. Medscape Emergency Medicine, 2009. (Accessed July 20, 2012, at http://www.medscape.com/viewarticle/589781.)
69. Zoghbi GJ, Misra VK, Brott BC, et al. ST Elevation Myocardial Infarction due to Left Main Culprit Lesions: Percutaneous Coronary Intervention Outcomes (abstract) In: Journal of the American Collegeof Cardiology; 2010 March 9; Georgia; 2010. p. E1712.
70. Kurisu S, Inoue I, Kawagoe T, et al. Electrocardiographic features in patients with acute myocardial infarction associated with left main coronary artery occlusion. Heart 2004;90(9):1059-60.
71. Engelen DJ, Gorgels AP, Cheriex EC, et al. Value of the electrocardiogram in localizing the occlusion site in the left anterior descending coronary artery in acute myocardial infarction. J Am Coll Cardiol 1999;34(2):389-95.
72. Yamaji H, Iwasaki K, Kusachi S, et al. Prediction of acute left main coronary artery obstruction by 12-lead electrocardiography. ST segment elevation in lead aVR with less ST segment elevation in lead V(1). J Am Coll Cardiol 2001;38(5):1348-54.
73. Gorgels AP, Vos MA, Mulleneers R, de Zwaan C, Bar FW, Wellens HJ. Value
of the electrocardiogram in diagnosing the number of severely narrowed coronary
arteries in rest angina pectoris. Am J Cardiol 1993;72(14):999-1003.
74. Barrabes JA, Figueras J, Moure C, Cortadellas J, Soler-Soler J. Prognostic value of lead aVR in patients with a first non-ST-segment elevation acute myocardial infarction. Circulation 2003;108(7):814-9.
75. Kosuge M, Kimura K, Ishikawa T, et al. Predictors of left main or three-vessel disease in patients who have acute coronary syndromes with non-ST-segment elevation. Am J Cardiol 2005;95(11):1366-9.
76. Szymanski FM, Grabowski M, Filipiak KJ, Karpinski G, Opolski G. Admission ST-segment elevation in lead aVR as the factor improving complex risk stratification in acute coronary syndromes. Am J Emerg Med 2008;26(4):408-12.
77. Barrabes JA, Figueras J, Moure C, Cortadellas J, Soler-Soler J. Prognostic significance of ST segment depression in lateral leads I, aVL, V5 and V6 on the admission electrocardiogram in patients with a first acute myocardial infarction without ST segment elevation. J Am Coll Cardiol 2000;35(7):1813-9.