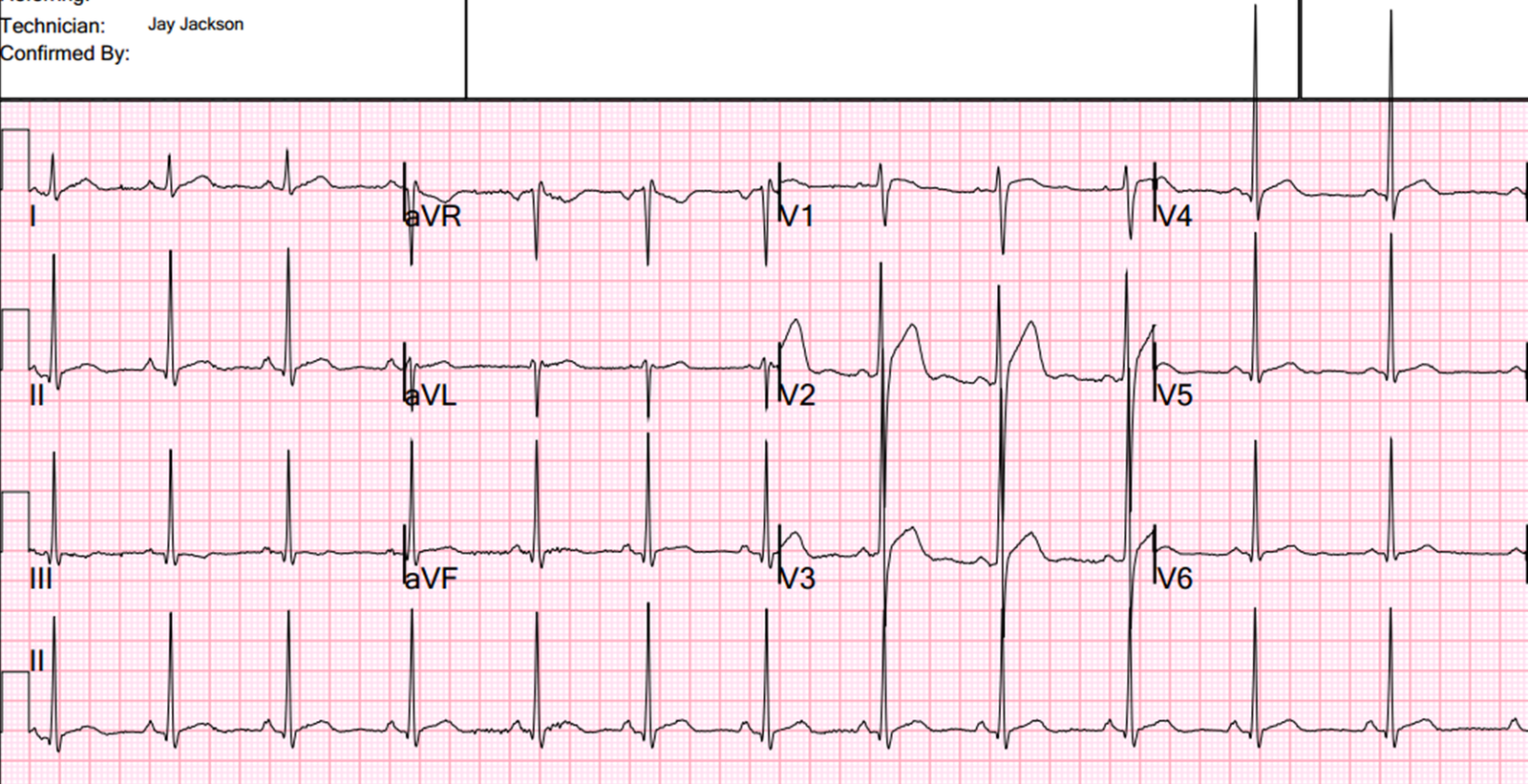
This is a male in his 50’s who was lying face down on the pavement stating that his chest was “killing him.” He stated it felt like his previous MI. H/o 2 prior stents. Skin was cool and clammy. He started to vomit. He had this prehospital ECG recorded at time zero:
 |
| No QTc is available on this. But in this case, you don’t need to do any analysis to determine if the ST elevation is normal variant or not. The PVC provides the diagnosis: it is an RBBB configuration (originating in the left ventricle): it has a qS pattern (not rSR’ because there is an initial Q-wave typical of old or new MI) and ST elevation. In RBBB, the ST segment should never be in the same direction as the terminal part of the QRS, as it is here. This is ST elevation of myocardial infarction. |
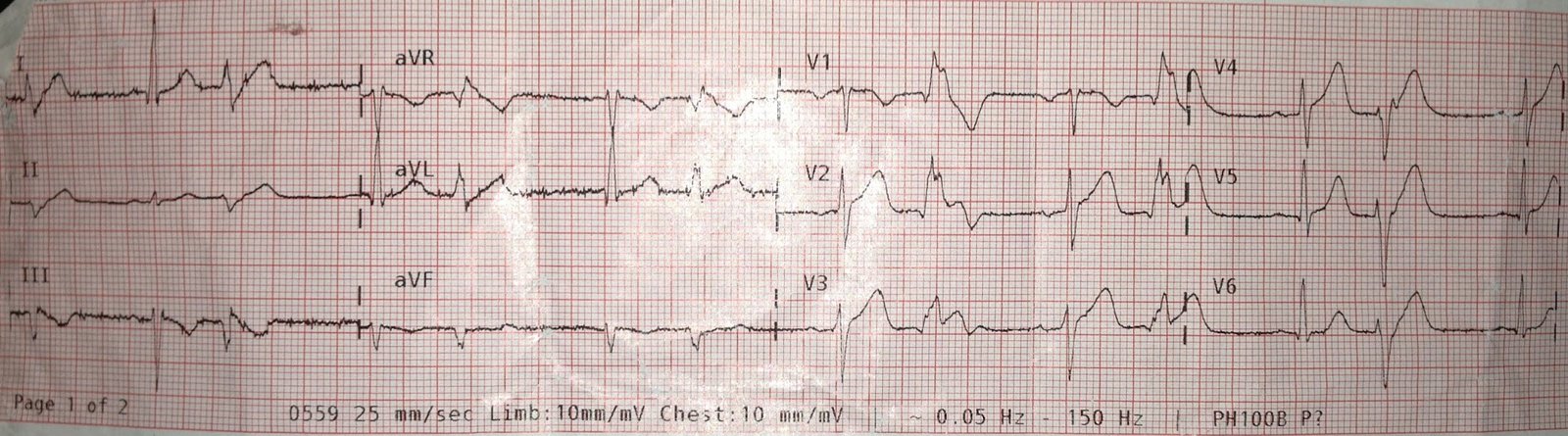
A follow up ECG about 15 minutes later was nearly identical except that there was no PVC:
 |
| I have estimated the QTc as 418ms. If you do not recognize this as STEMI, you can use the formula (STE60V3 = 2.5, QT = 418, RAV4 = 5.5) and you get 25.85 which is pretty much diagnostic of STEMI. |
The medic called in an anteroseptal STEMI and transmitted the EKG. To the chagrin of the medic, the ED MD thought that it was not a STEMI and did not activate the cath lab.
At t = 4 hours 15 minutes (255 minutes), the troponin returned positive and the patient was becoming hypotensive. He was taken for PCI of a 98% occluded LAD and 100% occluded circumflex.
The patient survived. I don’t have further info, but I suspect there was substantial myocardial loss.
Lessons:
1. Listen closely to the medics. They often know more about EKGs than you do (this message is for all emergency physicians and cardiologists).
2. Take advantage of all information. PVC’s often give you a lot of information. See also this case and this case.
3. Use the anterior STEMI formula. I have found since my study that it is incredibly accurate. I use it all the time to help confirm or refute my readings.