See this post for a wide complex that hides ischemic findings.
See this post for a difficult diagnosis in the context of a wide complex.
Case
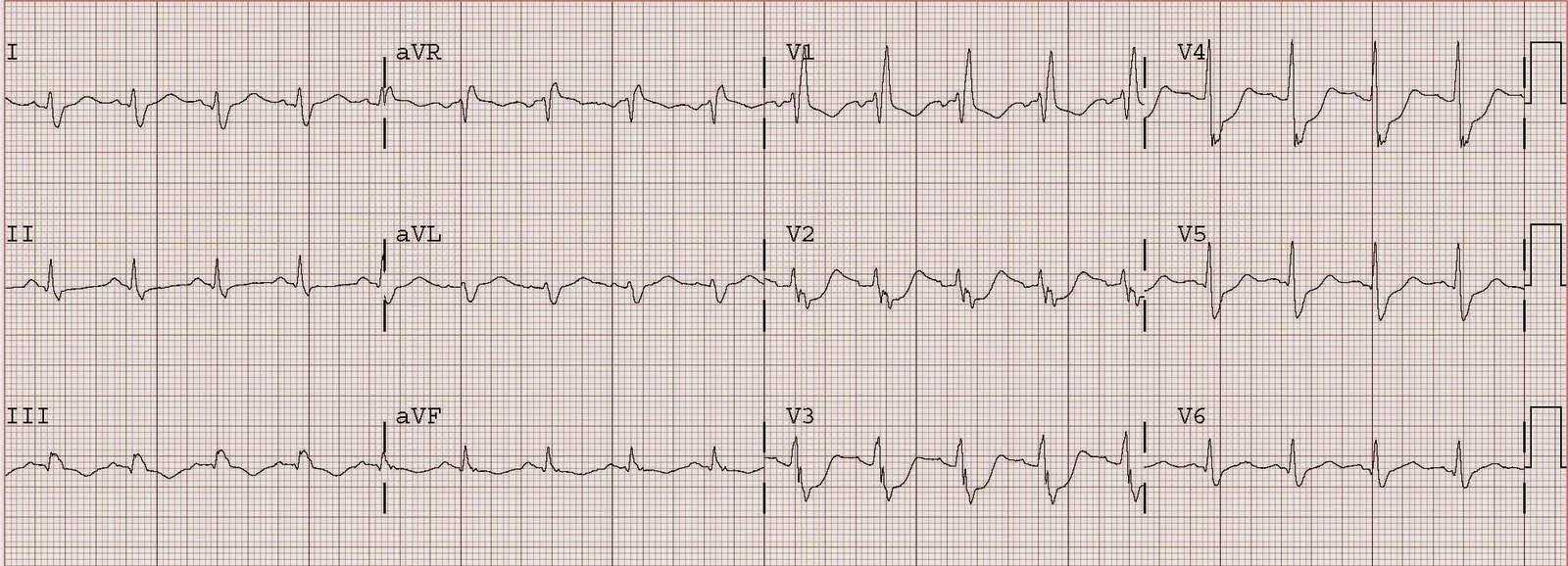
Here is a patient who had a cardiac arrest. Only approximately 25% of our atraumatic cardiopulmonary arrest patients have a STEMI (40% of v fib arrests) so the diagnosis of STEMI by the ECG is critical for the reperfusion decision. Here is the ECG:
 |
| The rhythm is atrial fibrillation. The QRS complex is wide, with a right bundle branch block but only subtle ST elevation in III and aVF, with very subtle reciprocal depression in lead aVL. The second complex in the ECG is a PVC, and is seen in leads I, II, and III. In leads II and III, in which the QRS of the PVC is predominantly negative (S-wave), there is marked discordant (opposite to QRS) ST elevation in leads II and III (inferior), far out of proportion to the preceding S-wave. I believe (without proof) that appropriate discordance in a PVC should be similar to LBBB, in which the average ST/S ratio is 0.10, and excessive due to STEMI is greater than 0.20. In lead I there is a positive QRS (R-wave) and reciprocal depression that is similarly discordant to the QRS and out of proportion. |
These PVC findings confirm the diagnosis of inferior wall STEMI in this otherwise difficult ECG.
The patient had an RCA occlusion.