A 70 y.o. woman who presented with L arm pain that started at 6:45 in the morning when she woke up. Pain was also in the upper back with some discomfort in the L chest. Described as “Achy” pain. She initially thought she must have slept wrong. No associated SOB, diaphoresis, or dizziness. No similar pain previously. No h/o CAD. She sat and rested but the pain got stronger, so she took 2 ASA. She felt a little “clammy.” The pain went away after ~15 min. She lay down for ~20-25 min and while lying down the pain returned and persisted x 10 min prior to resolving again. She called 911.
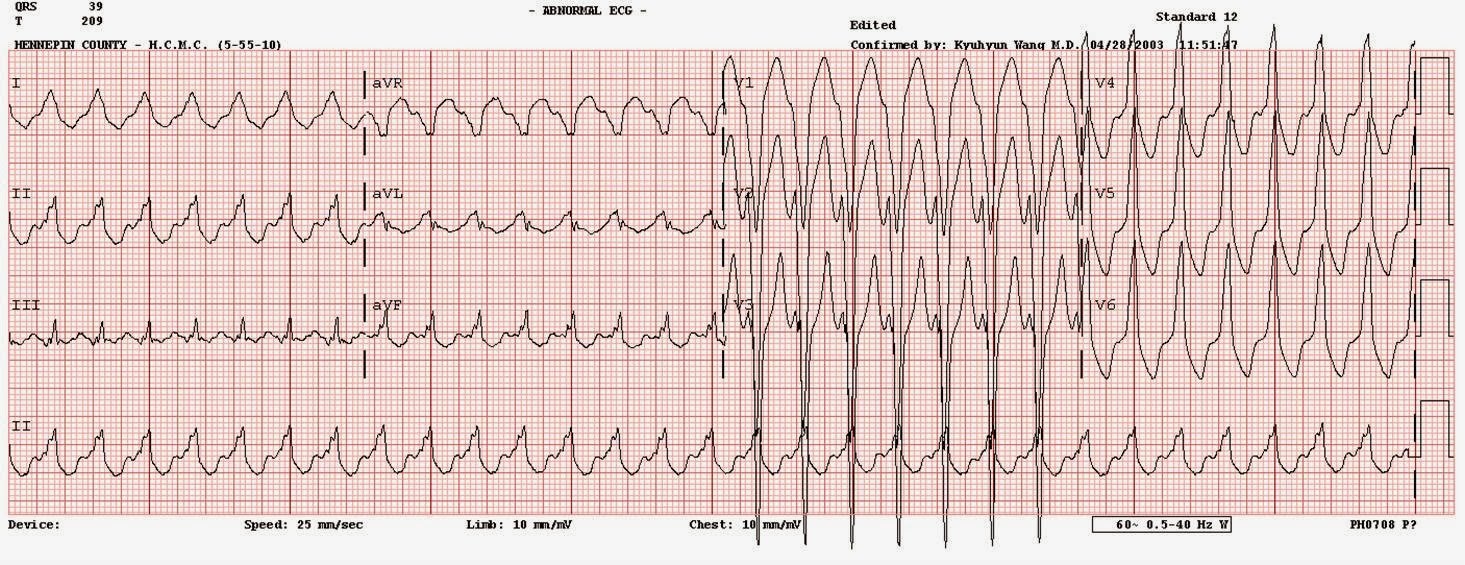
She was pain free when the medics recorded 3 ECGs over 40 minutes. They all were similar to the first:
 |
|
|
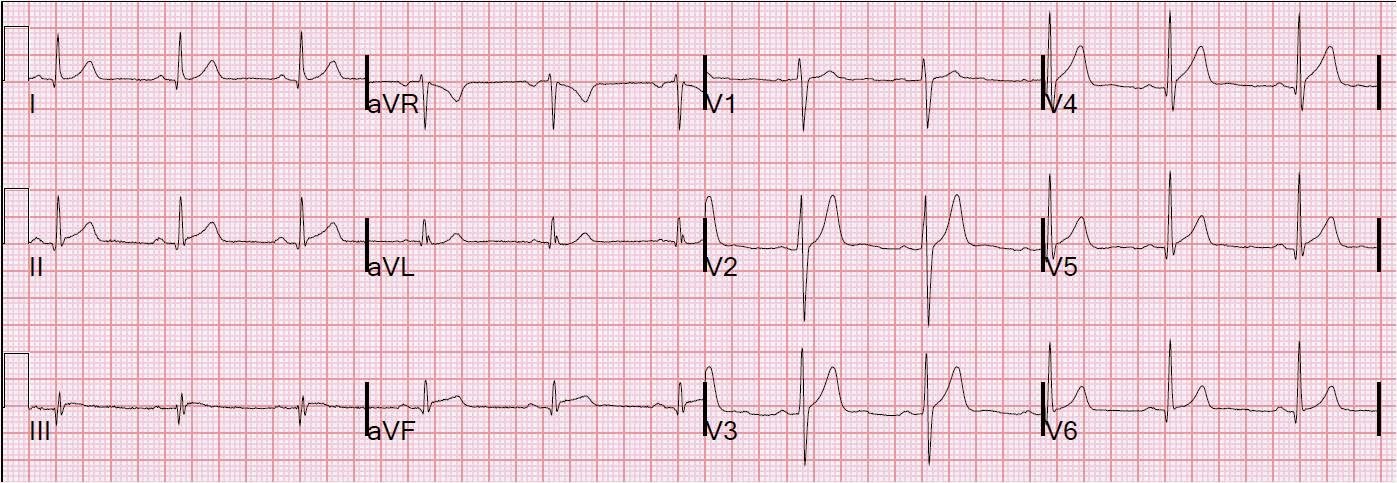
In the ED she was pain free. This was her ECG at presentation:
 |
|
|
look here for more on hyperacute T-waves:
https://drsmithsecgblog.com/search/label/hyperacute%20T-waves
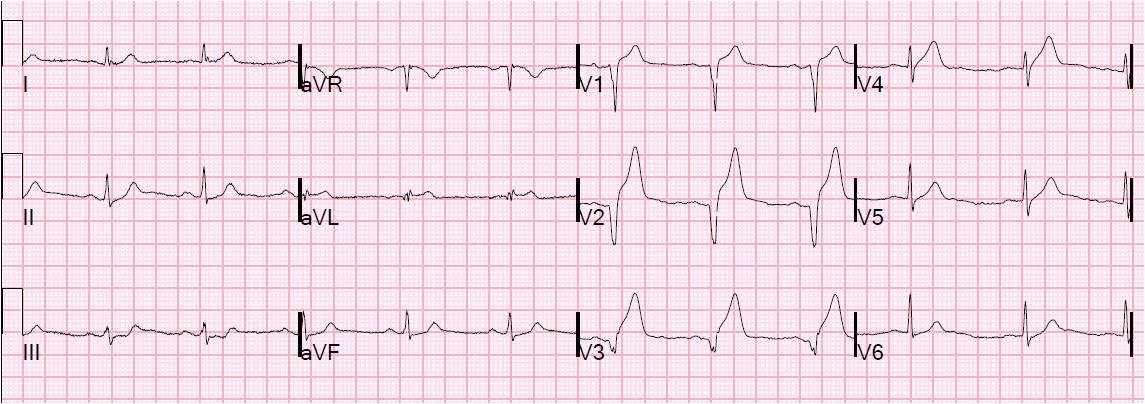
These ECG indicate that, at the time the patient was having pain, her LAD was occluded or nearly occluded. Old ECG from 3 years prior:
 |
|
|
So the patient has a spontaneously reperfused LAD. Antiplatelet and antithrombotic therapy was begun.
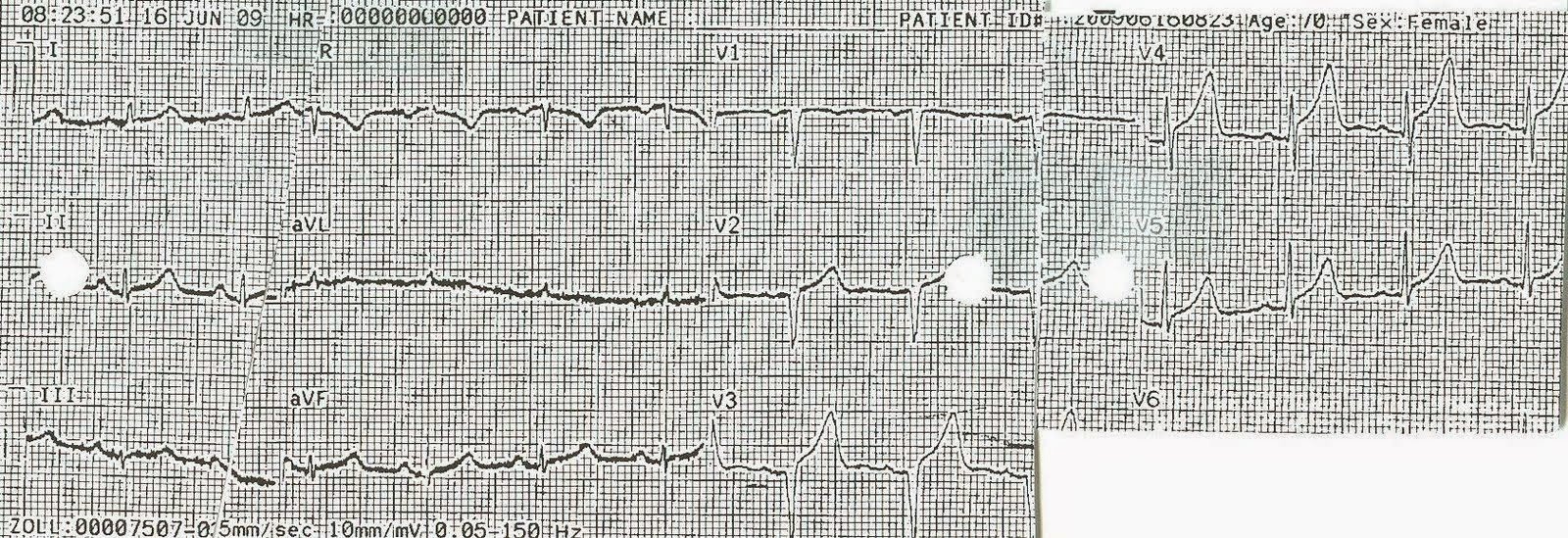
At 113 minutes after presentation (first troponin was less than 0.04):
 |
|
|
Just before cath, time = 240 minutes:
 |
|
|
Here is a composite of V4-V6 from previous to prehospital to ED:

2 hours after LAD intervention (80% stenosis with hazy LAD thrombus):
 |
|
|
Next Day. Troponin I peaked at 2.28 mcg/L. The septum, anterior wall, and apex are akinetic on echo (myocardial stunning):
 |
|
|
3rd day, 48 hours.
 |
|
|
6th day, 120 hours: Normal echocardiogram now:
 |
|
|
7 weeks later:
 |
|
|
3 months later:
 |
|
|
Summary:
1) With a large amount of myocardium at risk, there is a large wall motion abnormality
2) Hyperacute T-waves are a sign of a large amount of myocardium at risk and that it is still viable
3) With minimal actual myocardial cell death (infarction), as shown by a low peak troponin, the myocardium will recover:
a) The myocardial function (as shown by echo) will recover (this may take weeks)
b) The ECG will recover (this may take months, as in this case).