| A male in his early 30s was playing soccer when the ball hit him in the chest. At some point after this, he began having chest pain. The pain radiated into the L arm, and was 8/10 in severity. The pain was similar to pain he had with a previous STEMI, for which he received a bare metal stent in the LAD a couple years prior. He was on no medications.
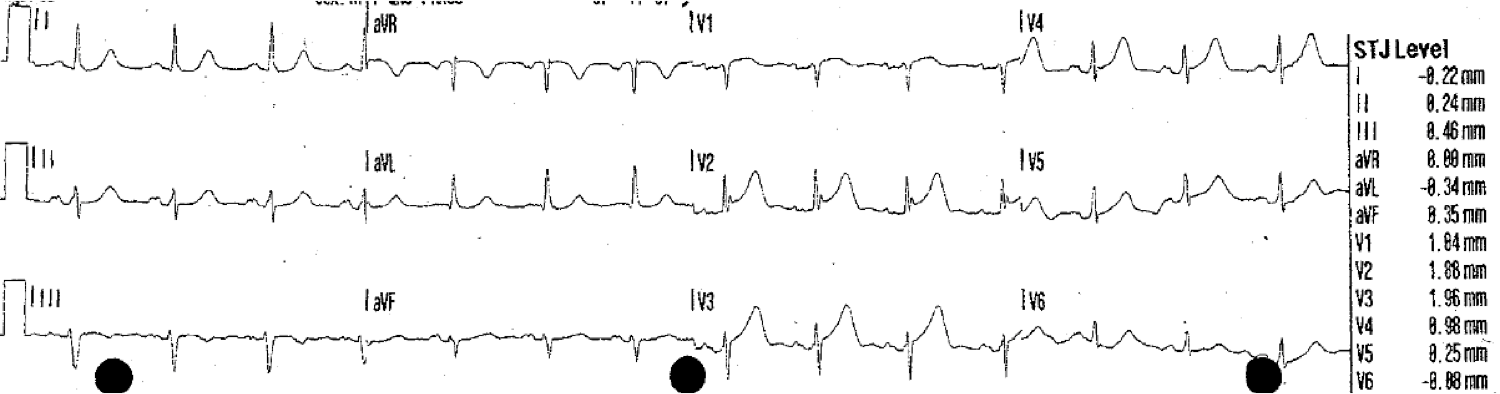
BP was 160/100. Here was his first ED ECG with 8/10 pain:
|
| There is sinus rhythm. There is minimal ST Elevation in anterior leads. There is a QS-wave in V2, due to the old anterior MI. The T-wave is taller than expected for old MI. In V4, the T-wave size is far out of proportion to the QRS. There is minimal STE in aVL with reciprocal ST depression in lead III. |
|
Here is the last ECG from 3 years prior:
|
| There are QS-waves in V2 and V3. The terminal part of the T-wave in V3 is inverted, and the T-wave in V2 is not tall. This is typical of LV aneurysm morphology (persistent ST elevation after previous MI) |

We have derived and validated a rule to differentiate “LV aneurysm” ST elevation from STEMI (just finishing validation manuscript). The rule depends on the principle that acute STEMI has a tall T-wave and LV aneurysm does not. There are two versions:
In the first rule, if there is any single T/QRS ratio in V1-V4 that is greater than 0.36, it is likely STEMI: for the ECG from 3 years prior, that would be lead V2. At 5mm/21mm, the ratio is less than 0.36 and would indicate LV aneurysm. But for the first acute ECG above, lead V2 is 8.5/15 which is 0.56 and would NOT indicate LV aneurysm.
In the second rule, one takes the sum of T-wave amplitudes in V1-V4 and divides by the sum of the QRS amplitude in V1-V4. A value less than 22 indicates LV aneurysm. In the second ECG from 3 years ago, that comes to 10/47 = 0.215, consistent with LVA.
Course
Records showed that his STEMI was anterior and resulted in an EF of 40%, an anterior wall motion abnormality, and peak troponin I of over 100 ng/mL.
He was given sublingual NTG with some pain relief. Here is the second ECG 13 minutes after the first, with 6/10 pain:
 |
| There is decreasing T-wave amplitude, consistent with some reperfusion. |
The cath lab was activated. The interventionalist did not think the ECGs were different from before, but he was glad to take the patient for an angiogram.
In the meantime, the patient was given aspirin, clopidogrel, and a heparin bolus. While waiting for cath, a NTG drip was started.
At 27 minutes after the first ECG, the patient had 5/10 pain on a Nitroglycerine drip at 200 mcg/min, with a BP of 130/80, and had this ECG recorded:
 |
| The T-waves are beginning to invert. This is consistent with some reperfusion. |
Outcome:
There was an in-stent thrombosis in the mid LAD with with 90% thrombotic occlusion and an embolism to the distal LAD. Plain old balloon angioplasty (POBA) was performed, and the patient was put on aggressive antiplatelet and antithrombotic therapy.
Here is the post cath ECG:
 |
| T-waves are fully inverted now. |
The troponin peaked at 12 ng/mL (not very high). The formal echo showed dense anterior, septal, and apical wall motion abnormality, with an EF of only 29%. This probably indicates “stunning,” and there will probably be recovery of wall motion and EF, as reperfusion was quick.
Stunning may take up to 6 weeks to recover.
Learning Points
1. T-wave height correlates with acute infarction.
2. Absence of tall or large upright T-waves in the presence of QS-waves correlates with large old infarction, or LV Aneurysm morphology.
3. Acute STEMI can be superimposed on LV aneurysm morphology. When it is, the T-wave turns upright with higher amplitude.