This patient presented with alcohol intoxication and possible overdose. No ischemic symptoms.
Rate 71
PR 224
QRSD 90
QT 424
QTc 461
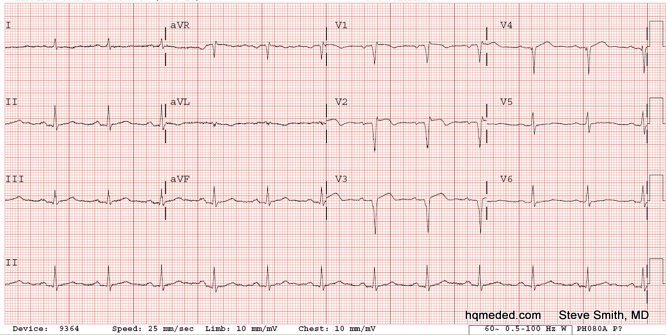
There is ST depression in V4-V6 (minimal). She is in alcohol intoxicated: high risk for hypokalemia.
Differential of ST depression is:
Secondary to abnormal QRS (LVH, LBBB, RBBB, etc.)
Primary ischemia
Hypokalemia
Digoxin
Normal variant.
This patient had a K of 2.8. Difficult case because she does not have prominent U waves (though they are there). I just finished a study of patients with proven hypokalemia compared to a control group. The QTc was the single best differentiator, with 450 ms the best cutoff. ST depression had good specificity but very poor sensitivity. Prominent U-waves were specific but not sensitive, and presence of any U-wave was sensitive but not specific. The best combination of factors was: Subjective diagnosis + QTc > 450 + Prominent U-waves, vs. none of the 3, with sensitivity of 86%, specificity of 100%, and accuracy of 92%. This held true when the subjective interpretation was done by residents who had had a short tutorial by me.