This case comes from a long term blog reader from Norway.
Case: 49 y.o male. No previous medical hx. 15-20 pack year smoking history. Parent with ACS in their 60’s. No DM. No HTN, no dyslipidemia, normal weight. Brought to the emergency department due to chest pain. Patient stated that 20 hrs before presentation he experienced numbness of the left hand, 1-2 hours after which he developed retrosternal chest pain ongoing from 02:00 lasting until 08:00 with no pain free period. Went to bed at 08:00. Awoke 11:00 pain free. The day of presentation, the chest pain started again while doing light physical work.
Pain free upon admission after NTG, 300mg ASA and morphine 2.5 mg given prehospital.
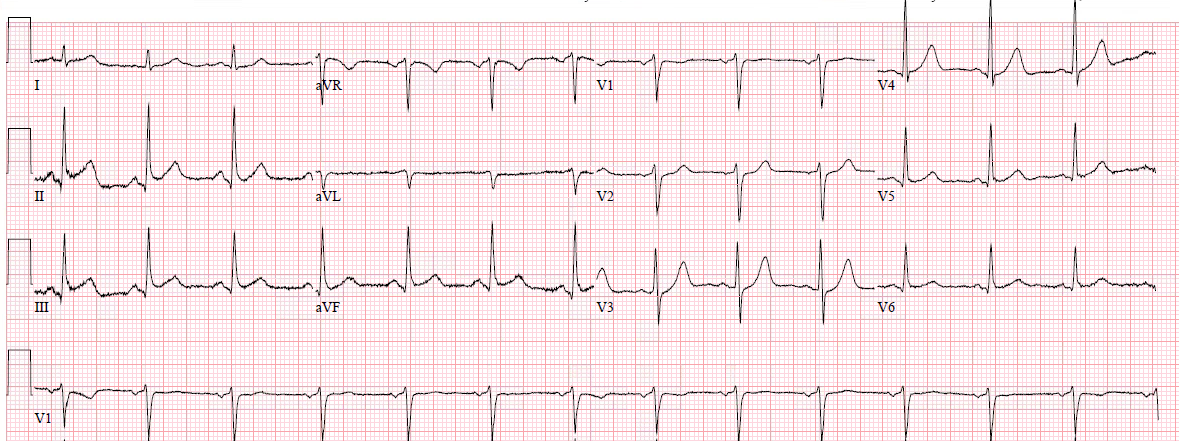
Here is the first ECG 1
I (Smith) am excluding limb leads as they do not add much and take up too much space.
 |
| Note: this is recorded at 50 mm/sec, the way they do it in Norway.
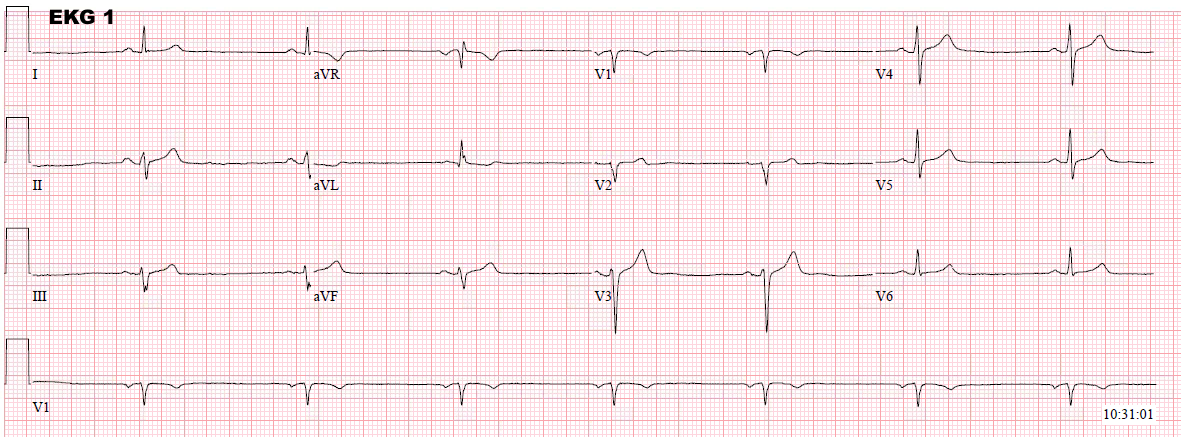
Below I have pasted the same ECG the way it would look at 25 mm/sec, which most of us are accustomed to: |
 |
| Not very worrisome |
“I could not see any ECG sign that had me particularly worried. I thought for a moment that the T wave in V3 seemed just a tad “fat”.”
“Physical Exam was unremakable. With a hx of ongoing chest pain for many hours with no pain free periods my concern for ischemia was dampened when the high sensitivity troponin T returned at 10 (ref value 0-14 ng/L).”
Repeat ECG (2, not shown) 30 min after first ED ECG was also without change dynamic change.
“I admitted him for observation. He was put on telemetry. The second troponin drawn 6 hrs later also 10 ng/L. He had no further episodes of CP. Telemetry without arrhythmia/ST-T changes.
Next day, the patient was pain free.”
“Due to worrisome symptoms, I went forth with stress test.”
ECG 3 was recorded just before the stress test and was not significantly different.
Stress test dynamic ECGs follow:
You need to press the play, but there is no arrow.
There is no change during this short timespan.
This ECG video starts 4 minutes into the stress test.
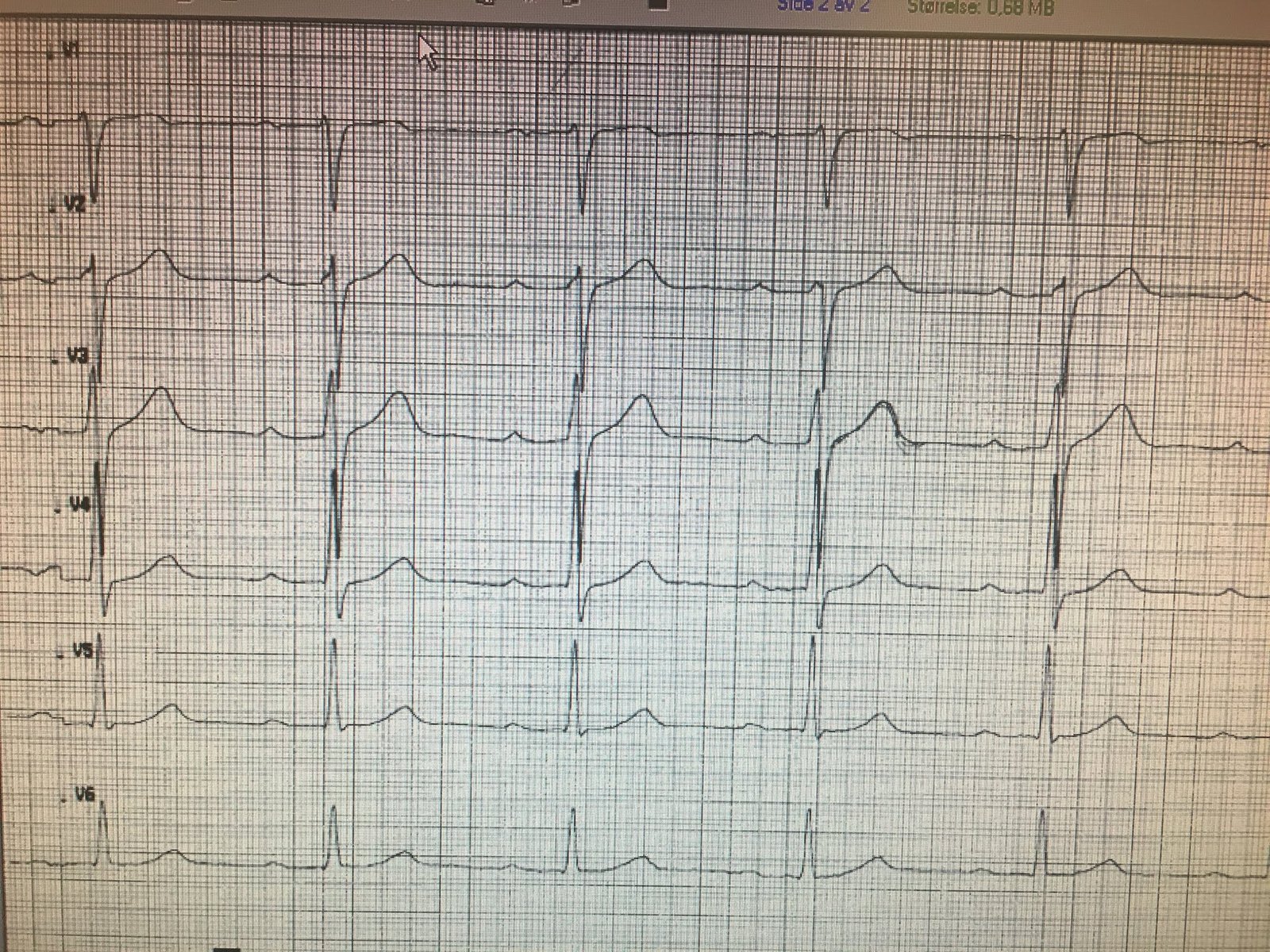
Pay attention to leads V3 and V4.
The entire video is 90 seconds, but you can speed ahead.
High ST Elevation develops.
The patient had no symptoms during this ischemia
This ECG was recorded immediately at the end of the stress test:

This was at 30 seconds after:

This was recorded at 1 minute:

This was recorded at 2 minutes into recovery:

This was at 10-15 minutes after end of stress test:

“The presenting ECG was without any obvious (at least to me) ischemic findings. The hs TnT was normal, even at 6 hours. But the stress test had impressive ST-elevation with rapid resolution. It is uncertain why he had no symptoms during the stress test; perhaps due to short duration of demand ischemia?”
“I cannot however explain ongoing symptoms for many hours prior to admission with normal high sensitivity troponin. Maybe enough blood flow as to not result in irreversible damage to myocytes?”
“Since the findings during stress test quickly resolved during rest, I felt quite confident angiography would reveal severe fixed proximal LAD stenosis, but I was not particularly worried about ruptured plaque.”
Comment: I (Smith) would be worried about ruptured plaque because the patient had presented to the ED with chest pain that was induced only by mild exertion and had also been present at rest.
“The patient was transferred to PCI-capable hospital same day. Troponin T after transfer was 16 ng/L. I thought they would find proximal LAD stenosis. They found severe mid-LAD stenosis distal to D2. The patient did well. Maximum trop was 69 ng/L after stent placement.”
Here are the angiogram images:
You can see the tight stenosis that is stented. It is wide open after intervention.
Notice the stent itself before contrast is injected.
Comment
Here is a relevant paper: Sandoval Y.
Apple FS. Smith SW. High Sensitivity
Cardiac Troponin Assays and Unstable Angina.
European Heart Journal: Acute
Cardiovascular Care 7(2):120-128; March 2018. Online published online on July
7, 2016 as doi:10.1177/2048872616658591